Published Date : November 28, 2017
Categories : OB/Gyn, Other Stuff
As a collector of old Ob/Gyn textbooks, I am absolutely amazed at some of the male chauvinistic gems they contain. Here’s a good one from 1934 (Thorek’s Surgical Errors and Safeguards):

He was discussing vaginal repairs, of course. The same author was wise enough to point out a couple of paragraphs later that “Many useless surgeries are performed for pecuniary reasons.” Sounds like it was a dangerous time to be a pelvic floor surgeon. I’d be willing to bet something else was going on that led to the two surgeons being killed.
Joel-Cohen, in his 1972 masterpiece Abdominal and Vaginal Hysterectomy, was kind enough to include as a separate insert a small tract for the “operating nursing sister” that taught her her role in performing an abdominal hysterectomy. The small, 15 page tract shouldn’t be too much of a bother for her to learn her place in the operating theater while the male surgeon read the full 170 page treatise. Therein he’ll encounter medical advice like this,
Thus the patient is admitted on a Sunday evening, has her operation on Monday morning, stitches out on Saturday and home on Sunday morning. I must admit that on numerous occasions, when the husband is a keen Sunday golfer, I discharge her on Saturday after removing her sutures.
Hmm. How nice. That being said, Joel-Cohen’s book is also full of brilliant advice and he was a pioneer in his time.
The 15th edition of Williams Obstetrics (1976) was edited by Jack Pritchard and Paul MacDonald, both from Parkland Hospital in Dallas. They were huge personalities and giants in their time. The 15th edition was a significant revision of the 14th edition, edited by Louis Hellman with Pritchard assisting. The 15th edition was all Parkland and is filled with a special type of arrogance. Collectors of these books will know that the 15th edition is remarkable for an entry in its index:
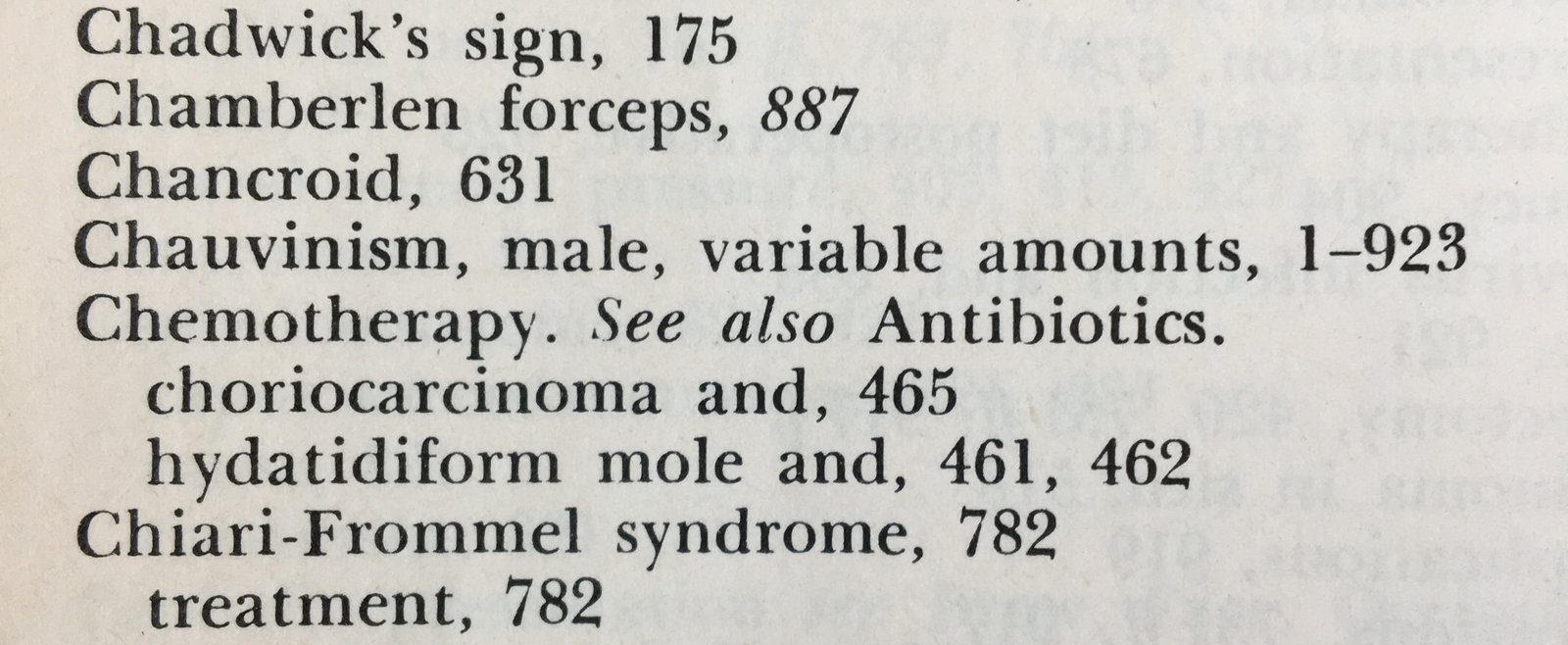
In case you are wondering, the book is 923 pages long. The keen index editor decided to qualify the entire text as chauvinistic. Pritchard and MacDonald were back again for the 16th edition in 1980 and so too was our furtive index editor:
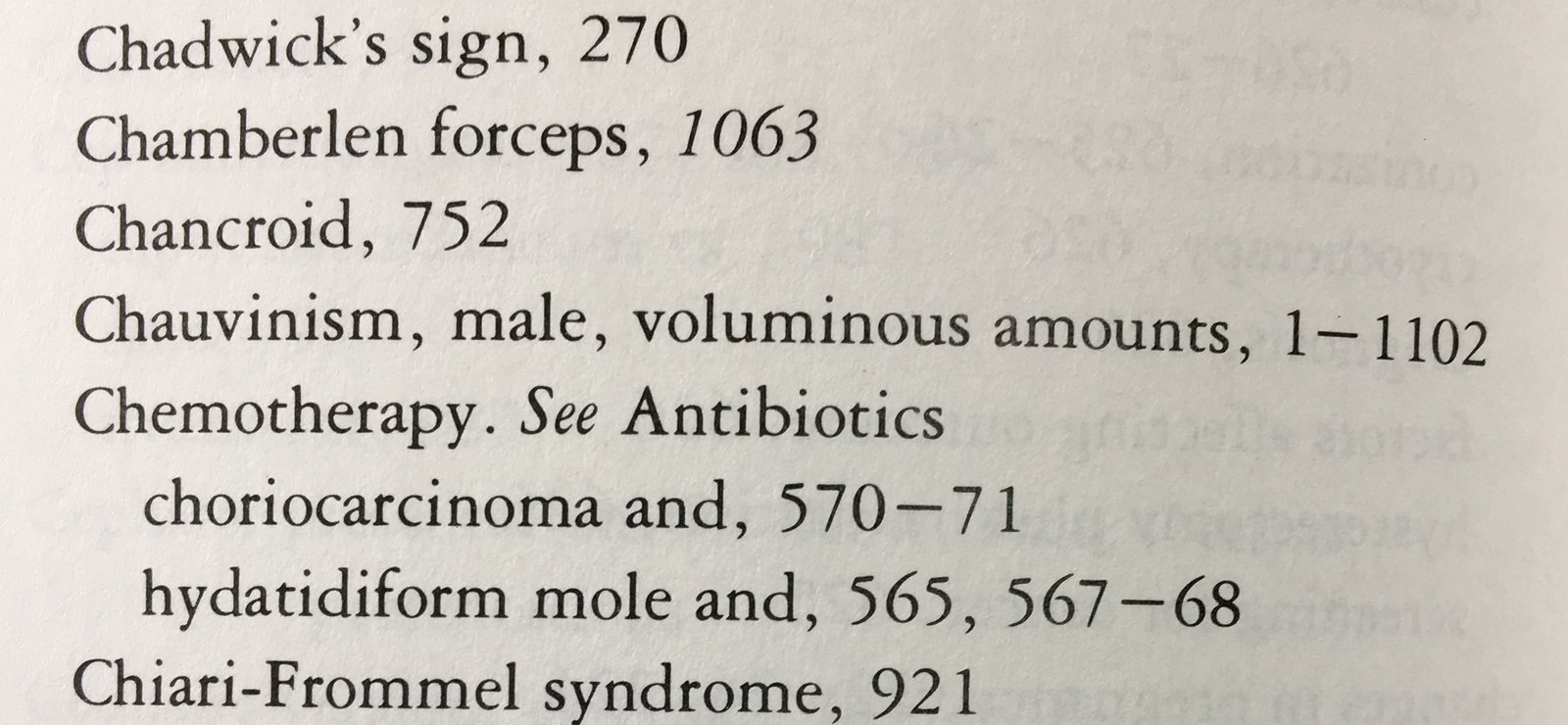
Yes, the book got longer and apparently the chauvinism more dripping. The mysterious index entry disappeared in the following 17th edition and Norman Gant was added to the authorship team.
So who was this crazed feminist that dared disparage Jack Pritchard’s work with these easter eggs? Well, apparently, it was his wife. In the preface to the 15 edition, the last paragraph reads:
Finally, no amount of thanks can express our gratitude to Ms. Signe Pritchard for her myriad contributions beginning with manuscript and ending (?) with index.
I’m not sure what the ‘(?)’ was for, but presumably he had written the preface before the index was finished so he was coyly hedging about thanking her for work she hadn’t yet done. I guess she got him back. Signe was thanked again in the preface to the 16th edition. In fact, Pritchard and MacDonald dedicated that edition to their wives (the prior edition was dedicated to doctors):
This edition of Williams Obstetrics is dedicated to Signe and Sue, whose love, loyalty, and devotion allowed us to pursue the careers that pleased us most–and whose patience, assistance, and criticisms renewed our dedication to do so.
I guess neither of them bothered to look at the index. I have no reason to dislike Jack Pritchard, but his personality was typical of his day. He was appointed Chair of the department at Parkland at age 33 when there was just one other faculty member and he built it into one of the preeminent departments in the nation. Maybe his wife was just joking. But do be careful with personality cults. More than anything, Pritchard (like Osler, Halstead, and Howard Kelly before him) was at the right place at the right time. But the bigger the personality, the more lingering the dogma.
For example, the authors recommended bed rest for the treatment of preterm labor. Why? Pritchard is credited with basically inventing evidence-based obstetrics. So one would assume that the recommendation of bed rest for preterm labor was based on scientific evidence. They tell us that the success of bed rest was, in part, attributable “to the reassurance of the mother that she is being treated.” In other words, calm the silly woman down with a trick and her body will behave. In the same chapter, they criticized the early studies that advocated magnesium sulfate for treatment of preterm labor, saying “the validity of the conclusions that were drawn are suspect.”
So, what’s the standard? Bed rest makes sense because it comports with the worldview that women are weak and when things go wrong in pregnancy it is due to their inherent weakness and inadequacy, but magnesium is not an effective tocolytic because Pritchard didn’t come up with the idea first? Like most texts of the era, there is good and bad but the fundamental view that men were saving poor little damsels in distress was omnipresent.
Recall that preeclampsia was once called toxemia because it was thought to be a build-up of toxins in the maternal blood that had not been secreted through the normal monthly purification of the menstrual cycle. Miscarriages must be caused by the woman doing something she shouldn’t have done, like picking up a bag of groceries. Bottle feeding was superior to breast feeding because men had used science to outsmart the female breast. In fact, for about half of the twentieth century, obstetrics consisted of rendering pregnant women unconscious, cutting a procto-episiotomy, and ripping the child out with forceps. Sounds very efficient and modern.
But surely we don’t think this way today. Have you ever recommended that a woman be on bed rest for any condition in pregnancy? Have you ever mocked a woman with a birth plan? Have you ever told a woman to “take it easy”? Do you believe that a Cesarean delivery is an improvement over vaginal delivery? Do you believe that when women suffer from depression or anxiety it is related to abnormal hormone levels? Much of the worldview of modern obstetric practiced was formed with the belief that women were inept and incapable and that science needed to fix them. Think about that next time you integrate old myths into your practice.
Published Date : November 22, 2017
Categories : OB/Gyn
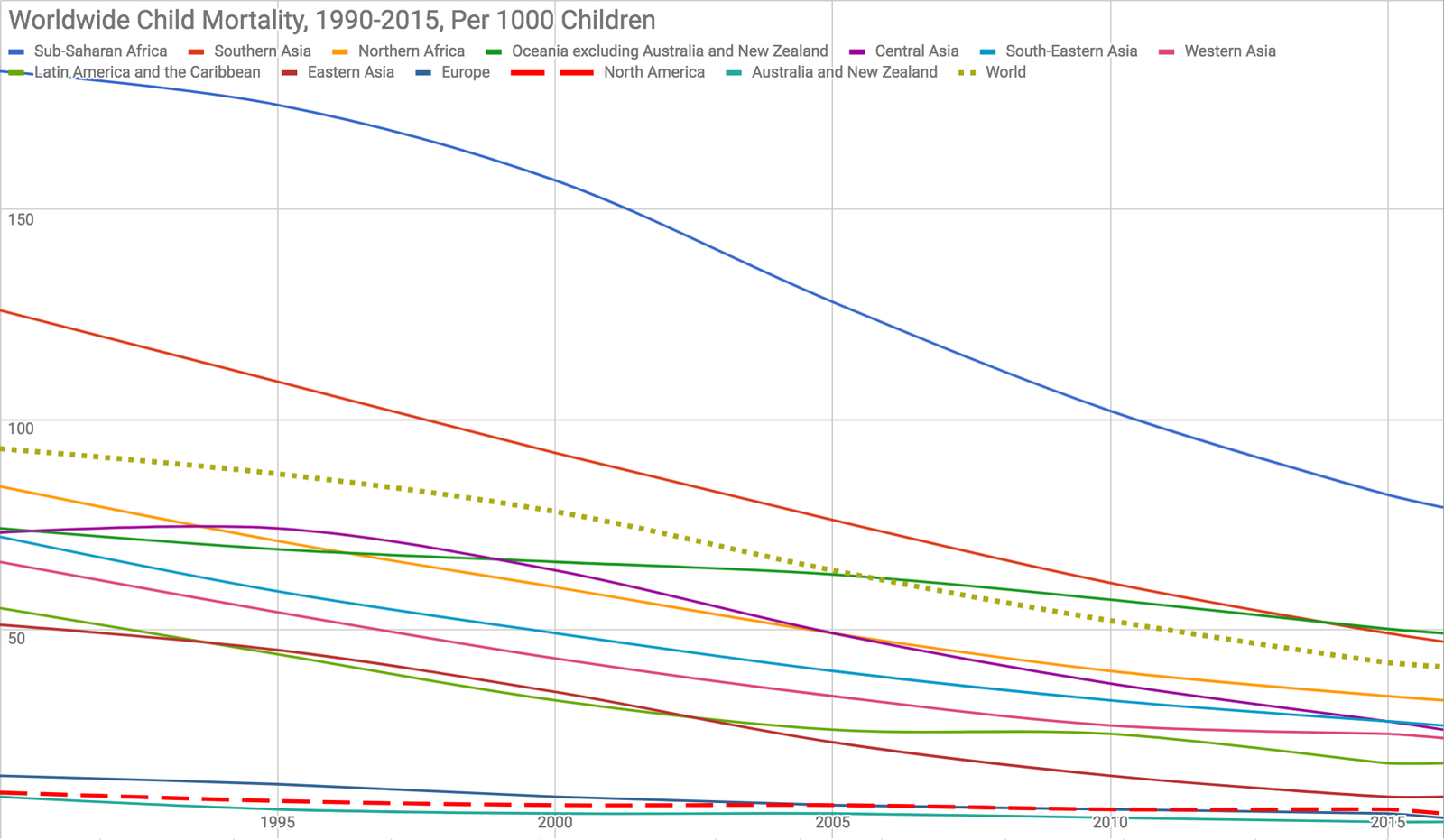
Ever heard of the Child Mortality Rate? It’s the number of children, per 1000, who die before the age of 5. This includes Neonatal Mortality and Infant Mortality, but it doesn’t include Fetal Mortality and therefore doesn’t include Perinatal Mortality. Confused? Here’s a refresher (each rate is reported per 1,000):
When you hear about how horrible the United States healthcare system is, it is usually related to our dismal infant mortality rates. Look at this hit piece in the Washington Post, for example, headlined: “Our infant mortality rate is a national embarrassment.” We are told over and over again that we are the worst among the wealthy nations, just 27th in the world, for infant mortality. We even lag behind economically-depressed Slovakia!
So what gives?
More importantly, how can we have such horrible Infant Mortality but very good Child Mortality? Notice the graph above: the United States has a Child Mortality rate that is bettered only by Australia. Yet, at the same time, we are told that our Infant Mortality rate is double that of most European nations, even though they lag behind the US in Child Mortality. How can this be?
To understand the problem, you have to think a little bit about how each metric can be manipulated.
If you think none of these things happen, you’re wrong. Infant Mortality and Perinatal Mortality have become such important markers of public health and funding and the resources that go along with it that countries around the world play games with these data.
For example, Japan has the lowest Infant Mortality rate in the world. How have they accomplished this? If you look casually, you will see claims of universal access to care and how wonderful and efficient their healthcare system is (though, in reality, it is heavily discriminatory against the poor). But what do they really do? Well, in Japan and Hong Kong, if a child is born alive but dies within the first 24 hours of life, it is considered a stillbirth, not a neonatal loss. This lowers the Neonatal, Infant, and Child Mortality rate, and does so dramatically since such a large fraction of children die in that window of time. Also, abortion is huge in Japan. The birth control pill was only introduced in Japan in 1999 and condoms and abortion have been the main methods of birth control for decades (abortion has been legal since 1949 and completely culturally accepted). This means that most fetuses with suspected anomalies are terminated in Japan (this is not the case in the US), leading again to fewer deaths across all the metrics since a large portion of fetal, neonatal, infant, and child deaths come from congenital anomalies: aneuploidy, heart defects, renal defects, etc.
Most developed countries don’t count very low birth weight babies against their Neonatal or Infant Mortality rates (considering them miscarriages instead). For example, Germany, Austria, and Canada ignore infants born weighing less than 500 grams, but we do not in the US. Mortality in this group of small babies approaches 90%. Switzerland some other European countries don’t count births of babies under 30 cm (or about 12 inches) in the Neonatal Mortality category; these types of inconsistencies, poor data collection, and under-reporting abound all over the world and conspire to make even Russia look like it has better Infant Mortality than the United States. Walker Ray summarizes some of these points in this piece.
What causes of death contribute to our “high” Infant Mortality rate? The leading causes of death for infants in the US are:
The leading cause of infant death are congenital anomalies for which the only intervention to lower the Infant Mortality rate is more elective terminations. Most of the other causes (those in bold) are related to extreme prematurity, with the highest mortality in a group of very low birth weight infants that the rest of the world doesn’t even count.
So, how does the US really compare to the rest of the world in terms of Infant Mortality? Are we really worse than Slovakia? No. The truth is, we cannot answer the question precisely because of the differences in reporting and the other games played by countries around the world to give themselves bragging rights. What is clear is that we should not even consider international comparisons until there is consistent reporting based on clear-cut definitions, and reporting that focuses on specific causes of death, so that we don’t get hammered because US women are less likely to terminate a pregnancy than Japanese women, for example.
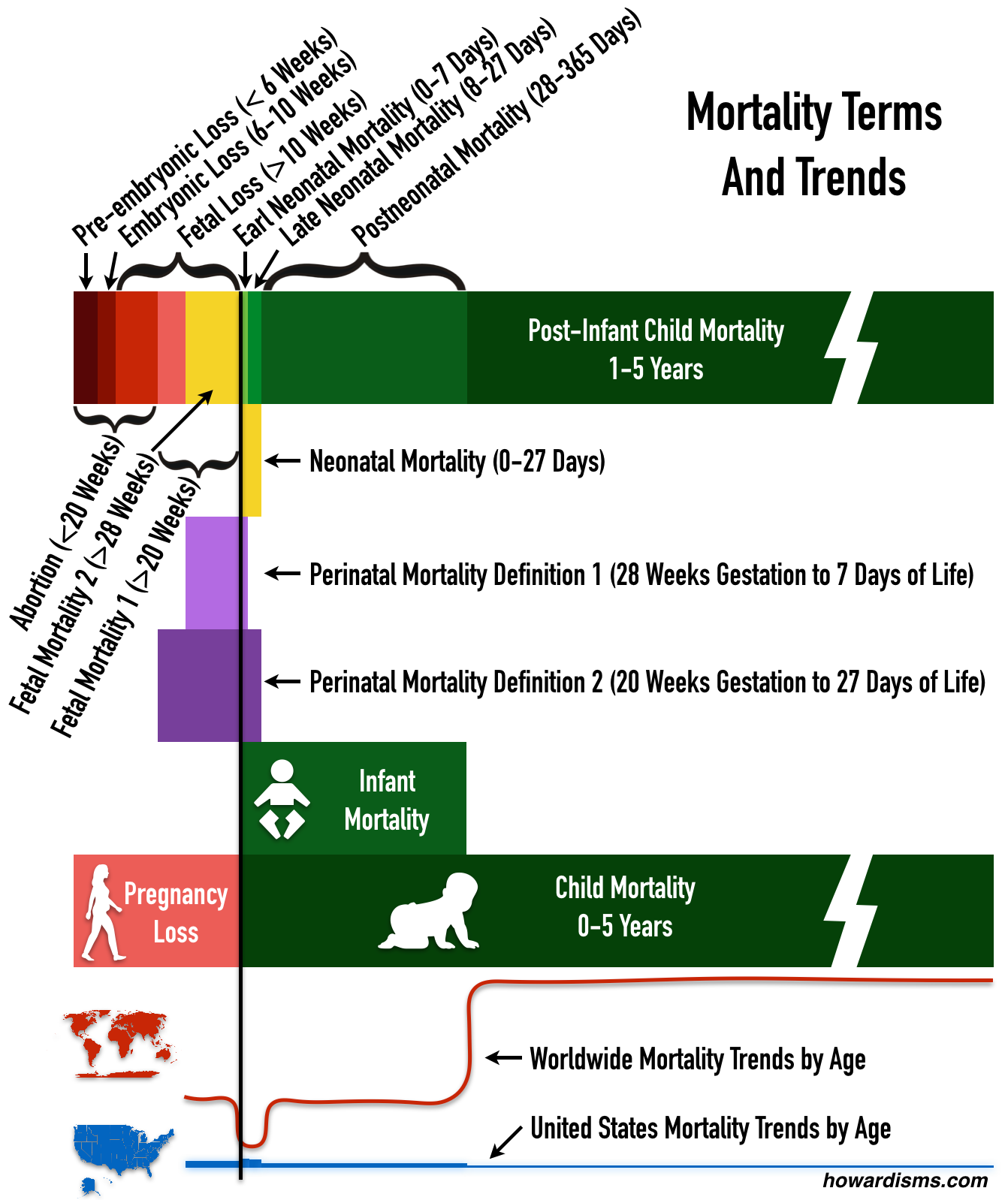
The graphic above shows how confusing the various mortality definitions are as well as the risk of death by gestational/neonatal age in the US compared to rest of the world. Notice that the highest rate of mortality in the US is in the neonatal period and more specifically in the first week of life. For the rest of the world on average, this is the lowest time period of death. How can this be? Because early neonatal deaths are transferred to the fetal period but kept in the neonatal period in the US. This has the effect of making the Neonatal, Infant, and Child Mortality rates all higher.
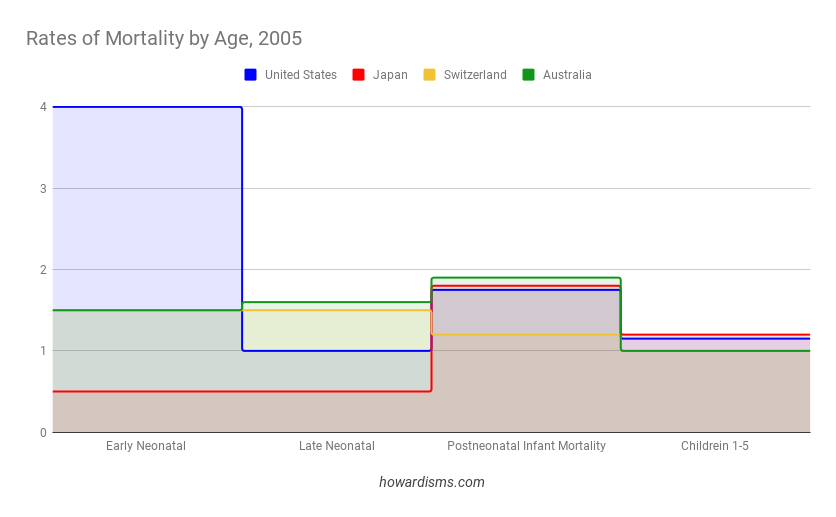
Notice in the above graph that the United States leads other low Infant Mortality countries in everything except Early Neonatal Mortality. This dramatic difference, all from the first 7 days of life, is the only reason why the US doesn’t lead the world. These regional variation in what counts as a neonatal death versus a miscarriage or fetal death, combined with high rates of elective termination of anomalous pregnancies, is the difference.
Child Mortality is, perhaps, a slightly more honest comparison. Because it accounts for all deaths before age 5, then any attempts to move deaths into different categories won’t affect the numbers. Northern American, as a region, is second only to Australia in most years when this metric is used. Child Mortality is still affected by incorrect counting of neonatal deaths (that is, shifting newborn deaths to fetal deaths). Correction for these reporting differences and controlling for differences in rates of women terminating anomalous fetuses would likely show the US to have the lowest Child Mortality Rate in the world. Even a metric that combined Fetal Mortality with Child Mortality would be problematic due to abortions and low reporting rates of miscarriages and terminations. A pregnancy ended in Japan for a diagnosis of trisomy-13 by cell-free DNA testing at 12 weeks might not have been terminated in the US and therefore would count towards such a combined metric.
One might argue that a good prenatal care system would emphasize detection of anomalous fetuses and early termination. But this is a value statement, not a scientific one. When we compare Infant and Child Mortality to other countries, what we mean to focus on are things like quality of obstetric care and delivery, neonatal resuscitation, penetrance of vaccination, access to emergency care and prevention of accidents, availability of clean water and food, and other public health measures.
International comparisons are unfair at best and dangerous at worst. They are used to inform fallacious policy decisions and typically manipulated for political purposes. Even comparisons among the US states is difficult due to some of the same factors that make international data collection problematic. The data is useful, but only as a sign of progress on state or regional level.
Remember this next time someone criticizes the US infant mortality rate. Later, we should talk about preterm birth rates and maternal mortality rates, because that’s a bit of a mess too.
Published Date : November 16, 2017
Categories : OB/Gyn
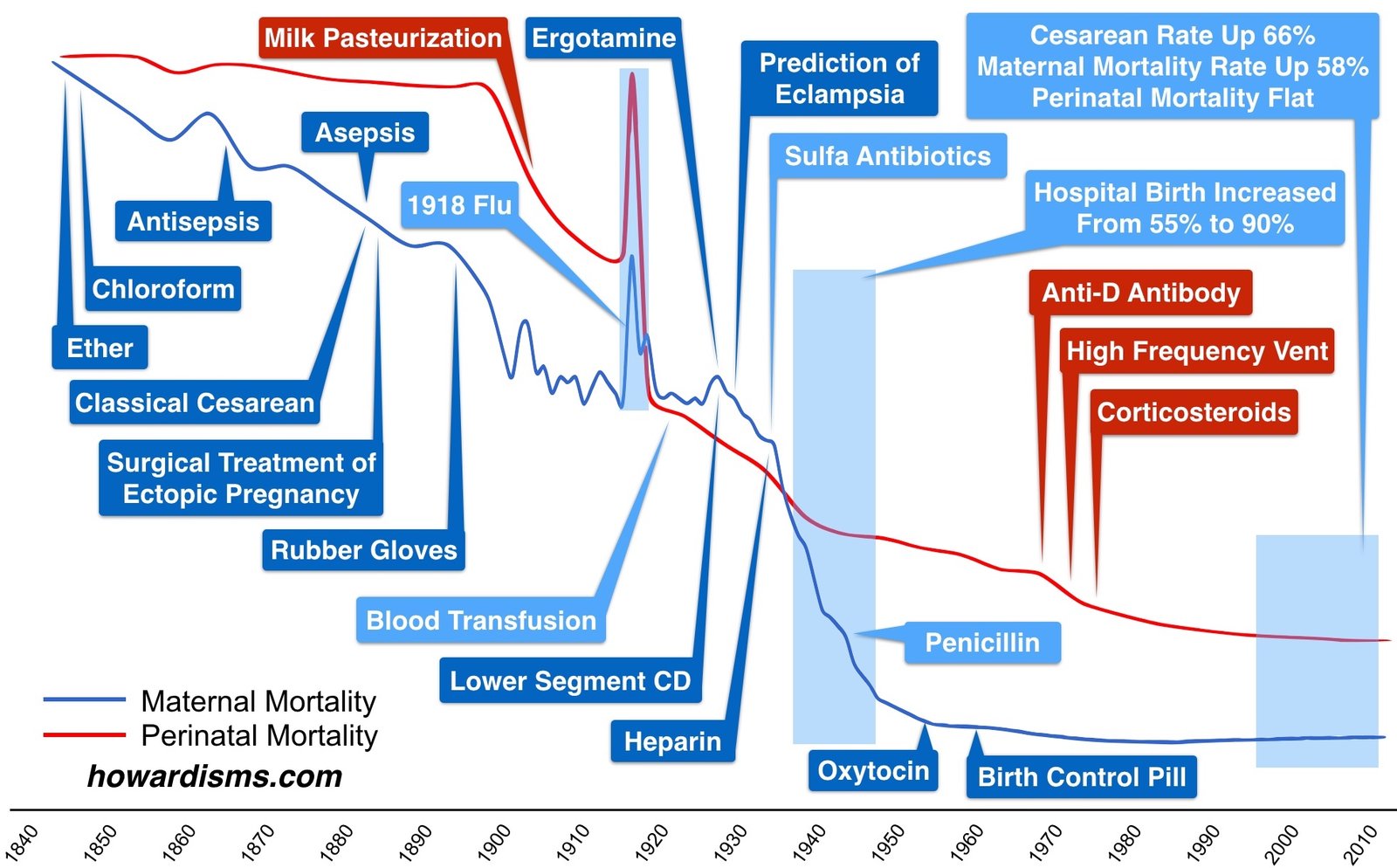
The graphic above shows the drop in maternal mortality since about 1840 (blue line) along with the drop in perinatal mortality over the same time (red line).
In the middle of the 19th Century, even in the Western world, a pregnant woman had about a 1% chance of dying during a given pregnancy; since there were no effective means of contraception, the average woman in America had about 11 pregnancies. This gave her a lifetime risk of around 1 in 8 or 1 in 9 of dying due to pregnancy. This rate of maternal mortality is still seen in some parts of sub-Saharan Africa today.

Women died in the past primarily of:
Take a look at some of the interventions that changed this:
The Spanish Flu pandemic of 1918 was horrific for mothers and babies and signals the importance of Flu shots (and other vaccines) today.
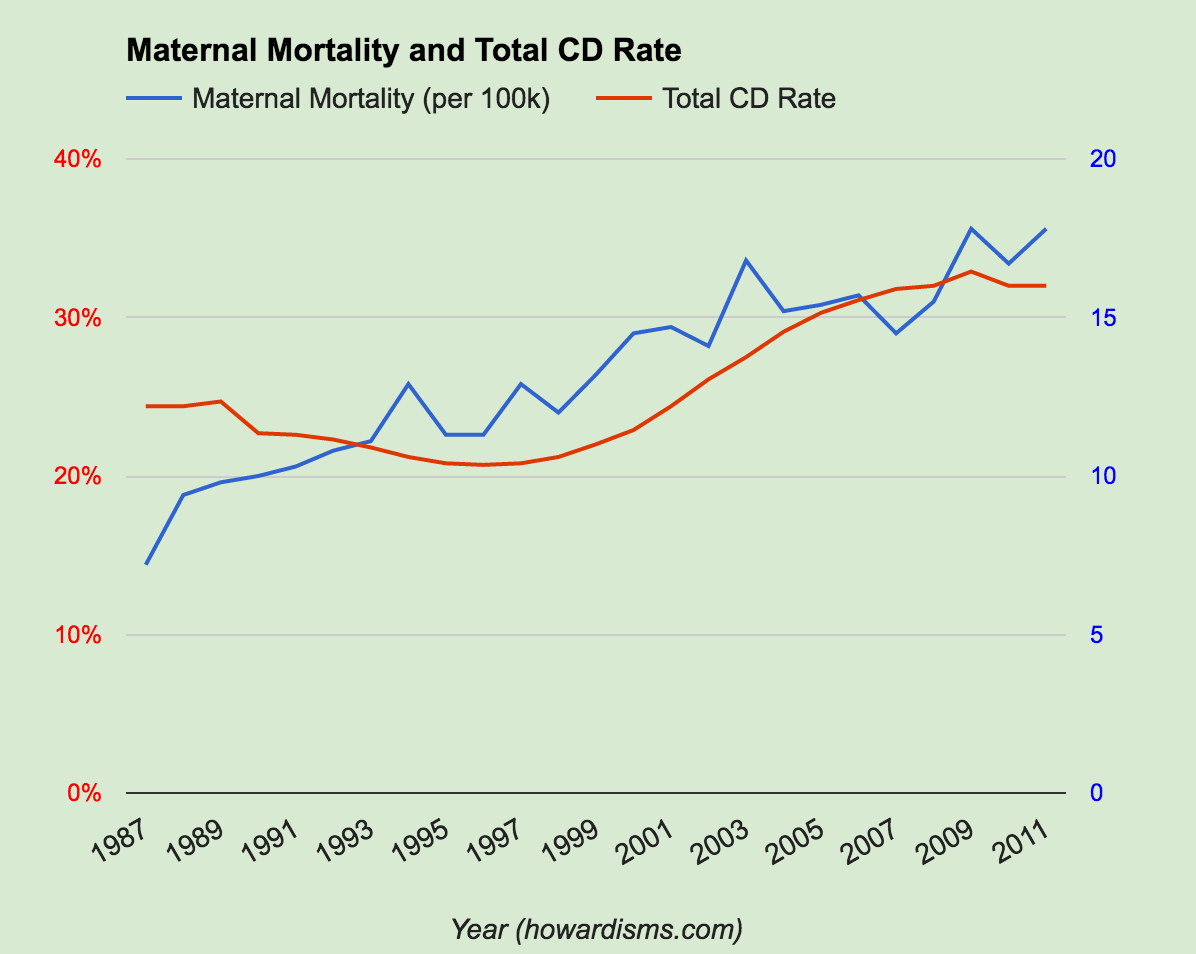
Unfortunately, you can get too much of a good thing. The over-utilization of Cesarean delivery over the last 30 years has led to an increase in maternal mortality since about 1987 with no attributable benefit to babies, but at an expense of an increase in maternal mortality since that year. Some of the increase is no doubt related to better reporting and classification of maternal mortality. The CDC started tracking this metric in 1986. But a lot of it is due to too many Cesareans, which increases the risk of maternal death due to infection, hemorrhage, and embolism.
Published Date : November 13, 2017
Categories : #FourTips, OB/Gyn

Hysterosalpingogram (HSG) is performed less commonly in modern gynecology than in the past, but it is still a valuable tool for some patients. A well performed HSG should be relatively painless and its results need to be correctly interpreted in context of what is already known about the patient. Here are four tips for performing an HSG.
1. Use a catheter.
Use a modern HSG catheter with an inflatable balloon tip rather than a reusable Cohen intrauterine cannula. Disposable catheters with a balloon can be purchased for about $15 or less and allow for the procedure to be performed with much less pain and discomfort than a traditional reusable cannula which requires a tenaculum to be placed on the cervix and instrumentation of the cervical canal in many cases. The balloon catheters are also more versatile in that they can be floated to different parts of the cavity or even placed intracervically (see Tip #4).
2. Beware of the false positives.
One of the most common reasons for an HSG today is to check for tubal patency. Office-based saline-infusion sonography (SIS), especially when combined with a 3D reconstruction, is very effective for providing views of the uterus and cavity and this study (so-called virtual hysteroscopy) has essentially replaced HSG for exploring uterine malformations, Asherman Syndrome, etc.
Thus, HSG today is commonly used to check for tubal occlusion following an Essure sterilization or to check for tubal patency as part of a workup of infertility. How accurate the test is will vary based upon the pretest probability of tubal occlusion for a given patient. Swart et al. determined that the point sensitivity for HSG (compared to chromopertubation) was 0.65 with a specificity of 0.83 for tubal blockage. Consider three patient situations:
Using the above sensitivity and specificity, the following positive and negative predictive values would be calculated:
 These numbers are very important and highlight one of the leading problems in clinical medicine: Incorrect diagnoses often occur because the pretest probability isn’t considered when determining predictive values of the test. If the patient has had an Essure and both coils are visualized in the appropriate location, then despite the rather high rate of tubal spasm that can occur with an HSG (about 1/3), the positive predictive value is still on the order of 99.7%. On the other hand, if the patient is being evaluated for secondary infertility and the test shows a blocked tube, the positive predictive value is only 61% (as compared to the gold standard of chromopertubation).
These numbers are very important and highlight one of the leading problems in clinical medicine: Incorrect diagnoses often occur because the pretest probability isn’t considered when determining predictive values of the test. If the patient has had an Essure and both coils are visualized in the appropriate location, then despite the rather high rate of tubal spasm that can occur with an HSG (about 1/3), the positive predictive value is still on the order of 99.7%. On the other hand, if the patient is being evaluated for secondary infertility and the test shows a blocked tube, the positive predictive value is only 61% (as compared to the gold standard of chromopertubation).
The real trouble happens when an HSG is done on an average, random woman who has nothing that would elevate her pretest probability for tubal occlusion. In this case, the result of blocked tube on HSG would carry only a 10.6% chance of actual tubal occlusion. Most of the apparent blocked tubes are the result of tubal or cornual spasm rather than true pathology. This statistic is particularly important as FemVue becomes more common in office practice.
FemVue (an agitated saline-infusion device) is used with ultrasound to test tubal patency in the office. It performs roughly as well as HSG when compared to chromopertubation in terms of sensitivity and specificity. The problem is that its use has been expanded in many cases to an inappropriate patient population. For example, some clinics perform it routinely on all fertility patients even if they have another underlying cause of infertility already established (like anovulation). In this case, the pretest probability of tubal occlusion (assume the woman has no history of chlamydia, etc.) is similar to that of a random woman. When tubal occlusion is noted on FemVue in a patient like this, the positive predictive value is close to 10%. So, in some populations, about 90% of positive results are false positives. This is a dangerous consequence of indication drift and a poor understanding of the role that pretest probability plays in determining the predictive value of a test.
3. Low pressure or high?
There are two somewhat different goals of HSG: to test the patency of the fallopian tubes and to visualize the contours of the cavity. Higher pressure of the contrast medium helps distend the walls of the uterus but is also more likely to cause tubal or cornual spasm, leading to a false positive result. So, a low pressure technique is more effective if the primary aim is to test the patency of the tubes, which is the most common objective of HSG. Inject the contrast medium at a slow and steady pressure and you shouldn’t need more than 2 or maybe 3 ml for the whole study. If the patient reports significant cramping, you are probably using a too much pressure (and that cramping may be associated with tubal spasm).
4. Try putting the balloon in the cervix.
Sometimes due to the acuteness of the uterocervical angle, the flexible catheter cannot pass easily into the endometrial cavity. Other times, the views of the cavity are incomplete because the tip of the catheter (and the balloon) are situated in the cornua and the contrast doesn’t distend the rest of the cavity well. Or, sometimes, the cavity won’t distend well because the contrast is leaking of the cervix.
In each of these cases, try this: place the catheter balloon in the cervix rather than the endometrial cavity, near the internal os, and inflate it. This will put the tip of the catheter in the lower uterine segment and the inflated balloon will occlude the cervical canal enough to force the contrast material upwards. This usually works and can make using a painful tenaculum unnecessary (either to pull on and straighten out the uterocervical angle or to try to occlude the cervical canal).
What else?
Use oil-based contrast instead of water-based contrast in infertility patients. Oil-based contrast is associated with a higher pregnancy rate. Beware of false positives associated with intravasation of contrast media into the parametrial vasculature. Do the test early in the follicular phase, particularly for fertility patients, to make sure that there isn’t an early, luteal-phase pregnancy.
Check out the video below for the basic technique:
Published Date : November 10, 2017
Categories : info, OB/Gyn
Hopefully none of these facts are surprising to you.

Published Date : November 6, 2017
Categories : Evidence Based Medicine, OB/Gyn

I hear it and see it all the time: caffeine causes fibrocystic change or at least makes the pain and breast tenderness associated with fibrocystic change worse. Hundreds of women have told me over the years that they avoid caffeine, at the advice of a physician, specifically for this reason. I’ve seen it in patient education information and a quick Google search will shows hundreds of “health” websites repeating this claim. It’s in dozens of health-related books. Some even claim that caffeine causes breast cancer. I’m sure many of my readers routinely tell their patients with breast pain to avoid caffeine as a treatment.
But is there any evidence that caffeine causes breast pain or fibrocystic breast changes? No.
Before we get to the evidence, let me editorialize for a moment. Medicine is full of these types of canards. Most of the advice and counseling given to patients is not based on evidence but is anecdotal at best and handed down casually from teacher to learner; the myths are therefore perpetuated. Remember this howardism to break the cycle: Never give a patient health advice that you don’t know to be true.
The story of this particular canard follows a typical pattern: a potential association is discovered in the data and a hypothesis is formed; the champions of the hypothesis are quick to draw conclusions that are not warranted by the data and the theory goes viral. The hypothesis enters medical practice before the hypothesis is actually tested. Eventually, the theory is subjected to more rigorous investigation and it is found to be untrue. By that time, however, it is so widespread into clinical practice that it has become “true” in most people’s minds and subsequent evidence is ignored or dismissed. Those who hold the hypothesis to be true just assume that there was once good evidence that supported it (even though there almost never was).
So let’s look at the evidence for this theory and where the popular belief originated.
The idea seems to have originated with the research of John P. Minton the 1970s. Dr. Minton was a surgical oncologist who studied breast cancer and potential breast cancer precursors. He died in a car accident in 1990 before much of his work was completed. He was also interested in decreasing the number of unnecessary breast biopsies for benign disease, and this (in his mind) meant decreasing how many women presented with fibrocystic change (fibrocystic disease as it was then called).
In 1979, he asked 47 women whom he had diagnosed with fibrocystic breast disease to stop using caffeine. Of those women, 20 quit using caffeine. Of those 20 women, 13 had resolution of their fibrocystic breast disease per Dr. Minton’s unblinded exam. This uncontrolled, unblinded study was the basis of the caffeine-causes-fibrocystic breast disease theory. Dr. Minton’s results were published in Surgery and in the American Journal of Obstetrics and Gynecology. A large amount of derivative literature was soon produced and fibrocystic disease was quickly added to books and other references about caffeine.
Note the pattern of rapid adoption of a hypothesis into medical practice before adequate study. Also note the typical poor quality of studies from the 1970s. A study of this type (13 patients) should hardly merit a poster presentation at a local science fair by a student, but in 1979 and 1980 it led to publication in two preeminent journals and fame for its author. Unfortunately, much of the “scientific” foundation of modern medical practices is rooted in similar quality evidence.
In 1982, Marshall et al. performed a case control study of 323 women with fibrocystic change and 1458 without and found no difference in their utilization of caffeine.
Rosenberg et al., in 1985, conducted a similar study of 2,651 women with breast cancer and 1,886 women without breast cancer and found no difference in the rates of caffeine consumption.
Ernster et al. published results of a randomized trial in 1982. They randomized 158 women with benign breast complaints and fibrocystic change to caffeine restriction or no dietary changes, and did mammograms before and after 4 months to objectively assess changes. They found no clinically significant changes and there was no differences in the mammogram aided diagnosis of fibrocystic change.
In 1984, Heyden and Muhlbaier performed another prospective study where 72 women were examined monthly over 7 months. Their symptoms, caffeine usage, and clinical histories were blinded to the examiners. The resultant exams showing fibrocystic changes were not correlated at all with the amount of caffeine consumption. The authors pointed out that a diseases that “waxes and wanes” as much as fibrocystic change is difficult to study without long term and blinded studies, which was an obvious knock at Minton’s methodology.
Lubin et al. in 1985 published a case control study in JAMA of 854 women with histologically diagnosed fibrocystic change or benign breast disease, 755 surgically diagnosed women, and 723 matched controls. Their evidence showed no correlation between caffeine consumption and benign breast disease.
In 1986, Heyden and Fodor published additional data from a five year retrospective study of 358 women with fibrocystic change and related coffee consumption. They concluded that “there is no scientific basis for an association between the consumption of methylxanthines and the development of fibrocystic breast disease.”
Later in 1986, Levinson and Dunn published a literature review of the evidence up to that point and concluded that “physicians need not recommend the avoidance of caffeine in otherwise healthy women who have fibrocystic breast disease.”
in 1988, Phelps and Phelps looked at data from 44 countries relating to breast cancer deaths and found that, if any association exists, caffeine was likely protective against death from breast cancer (though in fairness, it is doubtful that an association exists at all).
This was essentially the end of the literature relating to caffeine and fibrocystic breast disease because the issue was put to rest. But, as is usually the case with these types of stories, the myth did not die. The scientific evidence didn’t matter. Dozens of books have been written since then which are quick to cite the original article by Minton but no other papers. These reports do not view his study critically in any way. Thousands of websites report that caffeine causes or makes breast pain or fibrocystic changes worse and tens of thousands of doctors and nurse practitioners counsel patients about this “association” regularly.
There is far too much inertia in clinical medicine; for a field that is supposedly scientific, the majority of interventions and treatments lack a scientific basis.
While we are at it, how about Vitamin E for treatment of breast pain? Robert London reported in 1976 that he gave 12 women who had fibrocystic breast pain a Vitamin E supplement and 10 improved over the course of two months. This is the basis of the usage of Vitamin E for breast pain. In this case, London himself conducted a randomized trial in 1985 of 128 women which showed that Vitamin E was of no benefit. Nevertheless, Vitamin E is still commonly recommended as a treatment for breast pain.
A 2011 systematic review of treatments for breast pain found no evidence that evening primrose oil, pyridoxine, diuretics, progestogens, tibolone, antibiotics, combined oral contraceptive pill, a low-fat, high-carbohydrate diet, lisuride, or vitamin E reduced symptoms of breast pain or fibrocystic breast changes. Despite this, the ACOG Patient Eduction Pamphlet (AP138) “Fibrocystic Breast Changes” still recommends avoiding caffeine and cutting down on salty foods, especially the week before menses, and trying Vitamin E for treatment of breast pain.
Unfortunately, this phenomenon doesn’t just happen for relatively benign interventions like these. It happens for serious and consequential interventions all the time. Remember the pattern:
We could list numerous examples. I will cite magnesium for tocolysis as an intervention that fits this pattern perfectly (or use of progesterone for treatment or prevention of miscarriage or use of AMH to predict fertility). But if your interested in this topic, take a look at this 10 year review of 146 reversed medical practices (the list of each one is here). I will tell you which of the 146 no-benefit practices are related to OB/GYN:
How long before all these useless interventions go away? How about cardiac stenting, which just this week suffered yet another embarrassing reversal? Stents neither relieve chest pain nor improve mortality.
One trick is not to adopt practices before real evidence of efficacy, no matter how much it might make sense. Another is to give up practices as soon as evidence shows no benefit. Check out choosingwisely.org for more stuff you should not be doing (I have listed the obstetrics and gynecology ones in this article).
Published Date : October 29, 2017
Categories : OB/Gyn

My new book is now shipping! This is the definitive book for the definitive surgery and it’s just $39 so you have no excuse not to become a great vaginal surgeon!
If you’re one of the thousands of people who have used my YouTube videos describing the basic techniques of simplified vaginal hysterectomy with an energy sealing device, then you’re going to love my new book Simplified Vaginal Hysterectomy: An Evidence-Based Approach.
I present my new and simple method of vaginal hysterectomy which makes use of the latest scientific evidence in a refreshing and clear, straightforward style. This is not a stuffy textbook. The text covers every aspect of vaginal hysterectomy, including a comparison of the vaginal approach to other routes, indications and contraindications, relevant anatomy and tools, preoperative and postoperative care, the basic technique as well as advanced techniques with tips and tricks for the difficult vaginal hysterectomy, as well as prevention and management of complications.
The book also describes simplified techniques for procedures commonly done at the time of vaginal hysterectomy, including anterior and posterior colporrhaphy, culdoplasty, perineorrhaphy, uterosacral colpopexy, midurethral sling, cystososcopy, salpingectomy, and oopherectomy.
Using the techniques I describe, you should be be able to perform more than 90% of all hysterectomies through the vaginal route.
The appendices cover several important topics, including a unique and revealing view of the history of vaginal hysterectomy, a comparison of other vaginal techniques to those in the book, a description of the technique of laparoscopic-assisted vaginal hysterectomy, and a discussion of enabling technologies in surgery and how this relates to the use of energy sealing devices in vaginal surgery. Also there is a detailed analysis of how to become quicker in surgery and how to improve surgical education for residents, including a detailed competency-based curriculum for vaginal hysterectomy.
This book is a must for anyone who performs or teaches vaginal surgery. It includes over 70 full color pictures or illustrations and over 270 pages, with 9 chapters and 9 appendices. We have priced it inexpensively at just $39 so that every resident and gynecologist has a chance to read it. If you like vaginal surgery, you will love this book.
Order it directly here or from Amazon here.
If you are a program director, get a copy for each resident and will get you a discount (email me how many you need).
Published Date : October 25, 2017
Categories : Evidence Based Medicine

If you’ve never heard of the Antimullerian Hormone (AMH) Syndrome before, don’t worry: I just made it up. I’ll tell you what it is in a minute. But first, let’s talk about AMH.
AMH has been used by fertility clinics over the last few years as a test to determine ovarian reserve and predict fertility chances. A fertility clinic from Chicago says this:
Research shows that the size of the pool of growing follicles is heavily influenced by the size of the pool of remaining primordial follicles (microscopic follicles in “deep sleep”).
Therefore, AMH blood levels are thought to reflect the size of the remaining egg supply – or “ovarian reserve”.
AMH levels are used by fertility clinics in a variety of ways, but mostly to push women to more expensive interventions (like in vitro fertilization) earlier in their treatment course. The logic is that if a woman has a lower “ovarian reserve” she doesn’t have time to waste and should get to a definitive treatment as soon as possible. It has become a standard screening test in fertility clinics for this purpose. A “bad” AMH level weighs heavily on the minds of women who are already struggling with infertility and they will quickly skip interventions like intrauterine inseminations or other low-tech and less expensive options in the treatment armamentarium and run towards IVF, even if it means mortgaging the house. A physician friend of mine (who is ovulatory and has no history of infertility) had an AMH checked (apparently just because she is older); it was low and her physician talked to the REI who immediately recommended that she undergo IVF and have embryos frozen for future pregnancies since she would soon be menopausal. I guess it follows that if your AMH is low and you only have a few eggs left then soon you will become menopausal as the reserve is exhausted.
AMH levels have transformed fertility clinics over the last decade, changing the way that women are counseled about their fertility, and heavily influencing what choices they make for treatment.
There’s just one problem: there was never any science to support these claims. That may sound like an amazing statement; I am certain that you have been to a meeting and heard a talk where a respected physician told you how he or she uses AMH for these very purposes. You might even recall reading something about it or seeing it in a treatment algorithm. But, nevertheless, my statement stands: there was never any science behind it.
In 2002, de Vet et al. showed that AMH levels correlate with ultrasound-assessed antral follicle counts (AFC). It was also noted that AMH tends to decline year-over-year as women age (by about 5.6%, Bentzen et al., 2013). This work allowed nomograms to be developed which show that AMH levels increase in early puberty, plateau between ages 20 and 25, and then gradually decline towards menopause.
At the same time, other researchers noted wide intra- and inter-cycle variation (Wunder et al., 2007) and a large number of factors which might influence AMH levels like current (Dolleman, 2013) or past (van de Berg, 2010) oral contraceptive use, obesity, ethnicity, smoking, and differences in the AMH gene and its receptor.
Still, the basic science understanding of what AMH is and other observations led folks to hypothesize that it might be a good test to either predict time to infertility or menopause or the chance of pregnancy in infertile couples. When a hypothesis is generated, the usual next step is to test it; but too often in medicine, hypotheses are rushed into practice because it just “makes sense.”
However, finally this month an actual study was published which addressed the utilization of AMH levels to predict infertility. Steiner et al. studied 750 women and looked at serum AMH, serum FSH, inhibin B, and urinary FSH levels in women aged 30-44. They found that biomarkers associated with diminished ovarian reserve compared to normal ovarian reserve were not associated with reduced fertility. They also note,
Despite lack of evidence of their utility, biomarkers of ovarian reserve are being promoted as potential makers of reproductive potential.
So, ovarian reserve and fertility potential are not necessarily the same thing. Does that make sense? It doesn’t have to; it’s what the evidence shows. Studies have yet to show that a lower than expected number of ovarian follicles correlates with a decreased chance of future fertility. The authors found no difference in the time to pregnancy among the oldest group of women (38-44) with low AMH levels compared to normal AMH levels. More importantly, this paper doesn’t represent a change in belief or new and contradictory evidence; on the contrary, there was never any evidence that low AMH levels were associated with subsequent infertility. Physicians jumped the gun and started using AMH levels in an inappropriate way without sufficient evidence, harming women in the process.
Now we can define The AMH Syndrome. It is characterized by the following constellation of symptoms:
So, what are some other examples of the AMH Syndrome?
Fetal monitoring. Electronic fetal monitoring was first introduced into obstetrics with the promise of reducing the risk of cerebral palsy. Between 1958 and 1963, Edward Hon at Yale and Caldeyro-Barcia in Uruguay did the basic science research that allowed for the viability of continuous electronic fetal heart rate monitoring and also determined that delayed or late decelerations, as well as some types of bradycardia, variable decelerations, and diminished or absent variability, were associated with potential fetal distress. These basic science breakthroughs then led to conclusions not yet supported by clinical trials; it was naturally believed that if intrapartum fetal distress could be detected, then fetal outcomes could be improved. Physicians in clinical practice, eager to improve neonatal outcomes, started to embrace an idea that “made sense” and Hewlett-Packard, eager to make money, manufactured and sold the product. The patent-holders, eager to make a fortune, were all to happy to claim benefits not yet proven.
At first, fetal monitoring was used only on the highest risk pregnancies where the potential magnitude of beneficial effect would be the greatest, and soon both anecdotal and published reports of its potential life-saving benefit in that population were widely available. Then, due to therapeutic drift, the monitoring was extended to all pregnancies (and intermittent monitoring eventually became continuous). In retrospect, this practice has not decreased the risk of cerebral palsy, but it has dramatically contributed to the rising Cesarean delivery rate (and therefore maternal mortality) as well as the negative medico-legal climate of obstetrics. Today, even though evidence shows intermittent fetal monitoring is superior to continuous monitoring in average to low risk pregnancies, continuous electronic fetal monitoring continues to be used almost exclusively, creating a false but de facto standard of care.
Ultrasound. In the same way, over-utilization of obstetric ultrasound is another prime example. Where a biophysical profile (BPP) might theoretically reduce the risk of intrauterine fetal demise in a patient with preeclampsia, indication drift soon has the same BPP being applied to patients just because they are older than 35 or smoke cigarettes or some other indication for which no evidence exists. Both the manufacturer of ultrasound equipment and the physician make money off this expanded utilization, but the mother and baby are the ones who suffer due to iatrogenic prematurity, unnecessary inductions, and greater risk of cesarean delivery. Even clear-cut guidelines from our professional societies don’t stop over-ordering of BPPs, particularly in Maternal Fetal Medicine clinics whose funding is dependent upon over-utilization of testing.
Da Vinci robot. The da Vinci is another great example of The AMH Syndrome. There were no large prospective studies that showed that patients benefited from the use of the da Vinci system either in terms of outcomes or costs prior to its promotion from industry. The company obviously stood to make billions from large scale distribution of the robotic system and so did early physician champions, many of whom either worked for the company or sought to take advantage of the corporate marketing and distinguish their practices from their peers’ practices. Drift was fast and inevitable. Just because a da Vanci robotic hysterectomy might make sense for an ovarian cancer staging case doesn’t mean it makes sense for a benign hysterectomy, let alone a prolapse case. Today, it’s not uncommon to see it used for diagnostic laparoscopies or even sterilization procedures! Mature data consistently show that for almost all procedures for which the da Vinci is used, outcomes are not improved but costs explode. Still, so much investment has been made in training and equipment that physicians refuse to follow evidence-based recommendations for the appropriate use of the robot and consequently continue to mislead patients about purported benefits. Cheap plug alert: if you want to do hysterectomies in an evidence-based way, buy my book.
Magnesium sulfate. There are few better examples of the disconnect between science and practice than of magnesium sulfate tocolysis. Magnesium was adopted before any study showed improved neonatal outcomes and subsequently no study ever showed improved neonatal outcomes with magnesium tocoylsis but its use persisted and expanded. By 1991, the evidence was overwhelming that the practice was ineffective but it was still promoted by Maternal Fetal Medicine specialists. Long after the practice had been proven ineffective, new studies and trials were still being launched by those desperate for a false positive study that would justify its continued use. It never came. Finally, a new approach was taken: we won’t say we are using magnesium for tocolysis, we will say that we are using it for prevention of cerebral palsy (neuroprophylaxis). Study after study still failed to produce a significant result, but that evidence was ignored and marginalized until one subset analysis of a study showed a finding of marginal statistical significance and this finding, which was contrary to everything known about the topic and even the main conclusion of the study, was heralded as an important breakthrough by the true believers. The same physicians who accepted the most marginal evidence to argue for continued use of magnesium sulfate ignored follow-up data from the same study which showed no difference in childhood outcomes. But, recall, selective interpretation of evidence is a key feature of The AMH Syndrome.
Progesterone for miscarriage. The majority of obstetric providers recommend that patients check a progesterone level if they have had a history of miscarriage and consider progesterone supplementation if it is low (or even just empirically). There has never been any scientific evidence that progesterone supplementation will increase the live birth rate; despite this, the practice continues unabated. Each and every new study that confirms progesterone’s ineffectiveness is ignored. How is this financially motivated? Or, for that matter, how is the use of magnesium sulfate financially motivated? There are lot of conditions in medicine for which no good interventions exist. We have no intervention that stops preterm labor once it starts or that decreases the risk of miscarriage (in most cases). Patients are desperate and often willing try anything; doctors will distinguish themselves from other doctors by their willingness to try interventions that others will not and give hope where others have failed to. This earns those physicians more patients and that means more money.
There are tons of other examples where therapeutic or diagnostic drift occur without evidence because it is financially beneficial. How about routine urodyamic testing for simple stress incontinence? Universal first trimester screening? Universal diabetes screening? Mammography in the 5th decade in average risk women? Pap smears in women under age 21? Under-utilization of long-acting reversible contraception in deference to oral contraceptive pills? Over-utilization of DEXA scanning (particularly when the physician owns the machine)? Thrombophilia work-ups for women with a history of infertility or recurrent miscarriage? Ultrasound of cervical lengths after 24 weeks? Et cetera.
What other examples of The AMH Syndrome are you aware of? What do you routinely do in practice that has no basis in science? How about prophylactic salpingectomy? Were you even aware that there was never any science behind checking AMH levels to predict fecundity? If not, what does this tell you about how information is disseminated in our journals and meetings?
Published Date : October 16, 2017
Categories : Evidence Based Medicine, OB/Gyn

Simpson and assistants discovering anesthetic effect of chloroform
Next to Pitocin, obstetric anesthesia is probably the second-most hated intervention among the natural birth community. Like Pitocin, obstetric anesthesia is blamed for excess Cesarean deliveries and various other obstetric complications, and it is also claimed by many that women who undergo pain relief during delivery simply don’t bond with their children as much as they should or even love them as much as those mothers who don’t receive anesthesia during delivery. Doctors and hospitals are seen as pushing epidurals and pain meds on laboring women, leading to unspeakable ills.
The history of obstetric anesthesia is actually quite amazing, and is still relevant today in helping understand what we think about pain relief during labor.
One of the greatest differences between ancient medicine and surgery and modern medicine and surgery is the ability to control pain. As I discussed in the first appendix of my new book about vaginal hysterectomy, anesthesia before 1850 usually involved opium derivatives like Laudanum or simply alcohol (or both). Many cases involved nothing at all. Scottish obstetrician James Young Simpson first used chloroform on humans for anesthesia in 1847, administering it to a laboring woman after experimenting on himself. Two years before, in 1845, American physician Crawford Long administered ether to his own wife during labor. He had been experimenting with ether for a few years and began using it in surgery, but he didn’t publish his results until 1849.
The availability of anesthesia suddenly made surgery much safer and certainly more humane, and led to the emergence of a controlled environment that allowed for better hemostasis, aseptic and antiseptic techniques, and a dramatic decline in morbidity and mortality. Surgery became a science and a wonderful tool to improve our quality of life instead of a desperation-filled act of barbarity. It started with inhalation gases.
Nitrous oxide, laughing gas, or “factitious airs” as it was originally called, was first synthesized by Joseph Priestly in 1772. Humphy Davy, who experimented with the gas for a variety of uses, first noted that it might have an anesthetic quality in 1799 and published this result in 1800 after trying the gas on himself when he had pain after a wisdom tooth extraction. However, it was not until December 11, 1844 that Horace Wells famously used it on a patient while performing a dental extraction in Hartford, Connecticut. Wells killed himself in 1848, after becoming depressed and despondent when one of his patients died from nitrous oxide. Nitrous oxide didn’t induce a potent enough effect for major surgery, but the idea that a gas could be used as an anesthetic quickly led to the use of diethyl ether.
Crawford Long was a physician in Danielsville, Georgia. He had read Davy’s work about nitrous oxide and decided to try to use ether (because it was more available) in 1842 to remove a cyst from a patient’s neck. Long continued to experiment with ether for many years before he published his results in 1849 in The Southern Medical and Surgical Journal. William Morton made the first public demonstration of ether as a surgical anesthetic in October, 1846. A year before, in 1845, Crawford Long administered ether to his wife during her labor, making Caroline Swain Long the first woman to receive inhalation anesthesia during labor.
In 1847, James Young Simpson, the famous Scottish obstetrician, first demonstrated the anesthetic properties of chloroform. Simpson had been searching for a compound that might prove effective, trying various chemicals on himself and his assistants. He actually lost consciousness after inhaling the gas and luckily woke up the next morning. On January 17th, he first administered chloroform to relieve the pain of childbirth to a woman called Jane Carstairs, in Edinburgh. She was the wife of a physician and had a contracted pelvis due to rickets. Mrs. Carstairs’ first pregnancy had ended with fetal destruction after a three day, agonizing labor failed to produce delivery due to her contracted pelvis. The doctor had perforated the fetal head and removed the dead baby from the obstructed labor. In her second pregnancy, Simpson administered chloroform to her and the baby delivered on its own in about 25 minutes after she became completely dilated. She woke up in disbelief that she had delivered when she was presented her “own living baby.” Simpson went on to use chloroform for most of his laboring patients in the months that followed, publishing his results in the forerunner to the British Medical Journal. He said,
Obstetricians may oppose it, but I believe our patients will force the use of it upon the profession … I most conscientiously believe that the proud mission of the physician is distinctly twofold – namely, to alleviate human suffering, as well as preserve human life.
Simpson worked to popularize the use of chloroform as an anesthetic, not just for laboring women but for surgeries in general. He administered it to a four year old boy while his broken bone was set later in 1847. In the United States, in April of 1847, Nathan Cooley Keep administered ether to Fanny Longfellow, wife of Henry Wadsworth Longfellow, during her delivery. Critics of anesthesia sprung up immediately and Simpson spent a great part of the next several years of his career defending anesthesia on several fronts.
Surgery was viewed as so deadly that it was thought that adding something that weakened the pulse or sedated the patient would just lead to further deaths. To combat this notion, Simpson collected data on amputation patients and showed that only 1 in 3 died with chloroform compared to 2 in 3 without it. It was similarly argued that when used in childbirth, chloroform would produce higher risks of maternal morbidity and mortality (again with the general idea that “pain” was necessary to keep the patient vigorous); Simpson once against used data to show that this idea was wrong as well. Simpson was keen on using statistics and probability theory to aid in his medical decision making, a sentiment not shared by his contemporaries (or mine).
It was generally believed at the time that the pain of childbirth was natural and served a natural function; that God had created pain during the conduct of childbirth to make childbirth safer, and therefore removing the pain would necessarily make childbirth more dangerous. Harvey Graham, in Eternal Eve, found this quotation from the time about Simpson:
That he did not think anyone in Dublin had as yet used anesthetics in midwifery; that the feeling was very strong against its use in ordinary cases, merely to avert the ordinary amount of pain, which the Almighty had seen fit – and most wisely, no doubt – to allot to natural labor; and in this feeling he – the writer – most heartily concurred.
To which Simpson responded,
I do not believe that anyone in Dublin has as yet used a carriage in locomotion; the feeling is very strong against its use in ordinary progression, merely to avert the ordinary amount of fatigue, which the Almighty has seen fit – and most wisely, no doubt – to allot to natural walking; and in this feeling I most heartily concur.
Simpson’s breakthrough in the twin aim of alleviating suffering and preserving life was being criticized as unnatural just as today many of the extraordinary breakthroughs that have made humans live longer and better lives than at any point in human history are criticized as unnatural. The argument is made today that unless a woman experiences all of the pain in childbirth she cannot appreciate her child in the fullest nor love it completely; to which Simpson might point out that unless you write a letter by hand and carry it by foot to its recipient after fashioning the paper from raw material and creating the ink and pen from scratch, the recipient might not fully appreciate the message being delivered nor value it completely.
This idea is still promulgated among the “natural-birth” community. The (unfortunately) influential Michel Odent has said,
The pain of labor is part of the physiologic process … You cannot extract the pain and keep the rest. It’s a chain of events (quoted in Pushed by Jennifer Block).
There is, of course, absolutely no scientific basis for such a perverse claim, and one wonders if Odent just enjoys watching women suffer.
The last and biggest objection facing Simpson and other early practitioners of obstetric anesthesia was the idea that giving anesthesia specifically to women while they labored violated the biblical decree that women must suffer pain during childbirth as recorded in Genesis 3:16:
To the woman he said, “I will greatly increase your pangs in childbearing; in pain you shall bring forth children, yet your desire shall be for your husband, and he shall rule over you.” (NRSV)
The Church of Scotland had long since taken a stand against the use of anesthesia during childbirth. In 1591, a Scottish woman named Eufame Macalyane was pregnant with twins and sought some pain relief during delivery from a woman named Agnes Sampson. Because she attempted to provide pain relief to a woman in labor, Agnes Sampson was tried for heresy before King James; she was convicted, and burned to death on the Castle Hill in Edinburgh. Howard Haggard (The Story of Anesthesia) records one clergyman’s thoughts about Simpson:
Chloroform is a decoy of Satan, apparently offering itself to bless women; but in the end it will harden society and rob God of the deep, earnest cries which arise in times of trouble for help.
The same passage in Genesis that seems to demand that women suffer pain in childbirth goes on to state that men should toil and sweat and struggle with farming; but in the 19th century, air-conditioned tractors and harvesters had not yet been invented so men saw no apparent parallel. Simpson responded to the religious objections against obstetric anesthesia in an 1847 paper entitled Answers to the Religious Objection Against the Employment of Anesthetic Agents in Midwifery and Surgery. He pointed out several issues. He argued that, even then, farmers were using horses and tillers to make the work of farming easier; he pointed out that physicians should not attempt to save lives, since the same passage ends by stating, “For you are dust, and to dust you shall return.” He discussed the meaning of the Hebrew word translated pangs or sorrow and argued that toil or labor is a better translation; he further argued that since humans have a more difficult time delivering than other animals (due to the large head-to-pelvis ratio seen only in humans), then the principle of suffering is fulfilled. Simpson also argued that God himself used anesthesia when he caused “a deep sleep to fall upon the man, and he slept; then he took one of his ribs and closed up its place with flesh” (Genesis. 2:21).
Simpson methodically destroyed the various objections to anesthesia, both health and side-effect related and religious. But it didn’t matter. The medical community vilified Simpson and others who dared use chloroform. In 1848, The Lancet published a theologic response to Simpson’s paper written by a Dr. Ashwell, and the medical literature of the time was suddenly filled with theological papers and even papers written by Hebrew scholars about the meaning of the words in the verse.
For six years the debate raged on, until April, 1853. On April 7th, 1853, Queen Victoria was in labor with her eighth child, the future Prince Leopold, Duke of Albany. She asked Dr. John Snow to give her chloroform (which she received from him again in 1857 with the birth of her last child, Beatrice). Snow administered chloroform 77 times in his career to women in the second stage of labor, but it was this administration to the Queen that would largely silence the religious objections to its use.
Well, eventually any way. The initial response was one of disbelief and ridicule. On April 15th, a week later, the Association Medical Journal reported the birth:
We understand that chloroform was administered by Dr. Snow during the latter part of the labour, with very satisfactory effect; and that the Queen expressed herself as grateful for the discovery of this means of alleviating and preventing pain.
The responsible position, and the acknowledged skill of the physicians who sanctioned the inhalation of the chloroform, the Royal Majesty of the patient, and the excellence of her recovery, are circumstances which will probably remove much of the lingering professional and popular prejudice against the use of anaesthesia in midwifery, even when sanctioned by competent authority, and induced with requisite precaution. It is for this reason that we chronicle the recent accouchement of Her Majesty as an event of unquestionable medical importance.
Despite this early report, in the May 14, 1853 edition of The Lancet, the editors wrote a lengthy screed seemingly denying that chloroform had even been used on the Queen:
A very extraordinary report has obtained general circulation connected with the recent accouchement of her most gracious Majesty Queen Victoria. It has always been understood by the profession that the births of the Royal children in all instances have been unattended by any peculiar or untoward circumstances. Intense astonishment, therefore, has been excited throughout the profession by the rumour that her Majesty during her last labour was placed under the influence of chloroform, an agent which has unquestionably caused instantaneous death in a considerable number of cases. Doubts on this subject cannot exist. In several of the fatal examples persons in their usual health expired while the process of inhalation was proceeding, and the deplorable catastrophes were clearly and indisputably referrible to the poisonous action of chloroform, and to that cause alone. These facts being perfectly well known to the medical world, we could not imagine that any one had incurred the awful responsibility of advising the administration of chloroform to her Majesty during a perfectly natural labour with a seventh child. On inquiry, therefore, we were not at all surprised to learn that in her late confinement the Queen was not rendered insensible by chloroform or by any other anaesthetic agent. We state this with feelings of the highest satisfaction. In no case could it be justifiable to administer chloroform in perfectly ordinary labour; but the responsibility of advocating such a proceeding in the case of the Sovereign of these realms would, indeed, be tremendous. Probably some officious meddlers about the Court so far overruled her Majesty’s responsible professional advisers as to lead to the pretence of administering chloroform, but we believe the obstetric physicians to whose ability the safety of our illustrious Queen is confided do not sanction the use of chloroform in natural labour. Let it not be supposed that we would undervalue the immense importance of chloroform in surgical operations. We know that an incalculable amount of agony is averted by its employment. On thousands of occasions it has been given without injury, but inasmuch as it has destroyed life in a considerable number of instances, its unnecessary inhalation involves, in our opinion, an amount of responsibility which words cannot adequately describe. We have felt irresistibly impelled to make the foregoing observations, fearing the consequences of allowing such a rumour respecting a dangerous practice in one of our national palaces to pass unrefuted. Royal examples are followed with extraordinary readiness by a certain class of society in this country.
The editors simply could not accept that the Queen had chloroform or that her doctors could be such quacks. The editors of the Association Medical Journal replied on May 27 with this conclusion:
We would remind the Lancet that anaesthesia may be induced without loss of consciousness. To those accoucheurs who are in the habit of using chloroform in labour, we would refer, for final decision, the question of its being a safe or a dangerous practice. From a careful perusal of most of that which has been written on the subject, as well as from some personal experience of the practice, we may in the meantime state, as our own humble opinion, that the cautious inhalation of the vapour of chloroform during labour is entirely free from danger, and calculated to afford merciful relief from pain, in one of the most agonizing trials of humanity.
The explicit religious objections were not mentioned by the editors of The Lancet; instead, the objections were dressed up in non-scientific concerns about safety, particularly after the Queen had herself requested the medicine. But the safety concerns were a losing argument.
A year later, in 1854, the daughter of John Bird Sumner, the Archbishop of Canterbury, received chloroform during her delivery; finally, the religious objections seemed to be over. Well, almost. In the late 1850s, Prince Leopold, the child born to Victoria under the influence of chloroform, was diagnosed with hemophilia. He was the first member of the royal family to carry this diagnosis. In retrospect, Victoria must have been a carrier; the disease is X-linked. But as soon as Leopold received the diagnosis that would eventually take his life at age 30, many were quick to blame chloroform. Hemophilia was either a long-delayed side effect or the result of God’s curse upon Victoria for having her suffering alleviated.
Charles Meigs, in his textbook of Obstetrics from 1856, summarizes his objections thusly:
…never have I given, nor will I ever give any person chloroform…I am still quite convinced that the discovery of anesthesia in midwifery, has done more harm than good, and I believe its use will define, and not increase. I think it is declining already.
Boy, was he wrong. Soon, a variety of narcotics, often combined with scopolamine, gave rise to what was called “twilight birth.” Simpson was right; it was the patients who demanded and made obstetric anesthesia commonplace. The feminist movement of the early 20th Century actively worked to move pregnancy care from midwives to obstetricians, and from the home to the hospital. They also demanded that delivering women be given obstetric anesthesia, even as some of the obstetricians continued to question its safety, particularly the sedation of the newborn due to systemic narcotics.
Feminists and Suffragettes formed the National Twilight Sleep Association in 1914 to fight against the “primal curse” and “relieve one-half of humanity from its antique burden of a suffering which the other half of humanity has never understood.” Even more so than with inhaled gases, women became completely sedated and unconscious with twilight birth, and children did have an increased risk of neonatal depression. But safe general anesthesia, as well as spinal, epidural, and local anesthesia were eventually developed, which allowed women to experience the joy of delivery without the pain. It also allowed for safe operative vaginal deliveries and Cesarean deliveries, making fetal destruction a thing of the past and helping to relegate death during delivery to the history books. Ironically, many feminists today oppose obstetric anesthesia and the arguments against its use (false claims of safety issues, for example) are reminiscent of claims fought long ago by James Young Simpson. Certainly, not every woman wants or needs anesthesia; but for the majority of women, safe obstetric anesthesia has helped transform birth into a joyous event to be excited about, not a dreaded and dangerous inevitability.
Published Date : September 10, 2017
Categories : Evidence Based Medicine, OB/Gyn

Princess Charlotte of Wales
In the natural birth community, Pitocin is a dirty word. It is blamed, wrongfully, for nearly every ill that affects modern obstetrics: the high cesarean delivery rate, the pain associated with labor that leads women to want epidurals, postpartum hemorrhage, postpartum depression, fetal distress, autism, and just about anything else you can imagine. Some patients will do almost anything to avoid receiving some “Pit.” A quick Google search about oxytocin reveals countless horror stories and hysterical claims about the evils of this horrible medication that is a curse to modern women.
Pitocin, of course, is just a brand name for oxytocin. Oxytocin is made in the paraventricular nucleus of the hypothalamus and then released by the posterior pituitary. In 1954-1955, it became the first polypeptide hormone to be sequenced and synthesized. The American biochemist Vincent du Vigneaud won the Nobel Prize in Chemistry 1955 for his work on synthetic oxytocin. The commercial availability of synthetic oxytocin or Pitocin after the 1950s did radically change the practice of Obstetrics, but perhaps not in the way that many fear-mongers today claim.
To understand how it has changed Obstetrics, we first must understand what birth was like before so many interventions. Most patients who desire “a natural birth” long for the days before we started pumping dangerous chemicals into mamas and babies and interfering with and altering the natural process of childbirth. So here is a story to illustrate what birth was like before we screwed it up with so many interventions.
George III was King of Great Britain and Ireland, starting in 1760. At the time of his death in 1820, he was King of the United Kingdom and Ireland, as well as King of Hanover, which included territories that eventually became part of Germany.
George III was mentally unstable; “Mad King George” was thought to suffer from porphyria, and he had episodes of manic behavior and other irrational mood swings. The United States formed partly due to George’s madness. The US Declaration of Independence is essentially a list of his excesses. George was not liked very well in the United Kingdom either, particularly as his mental health deteriorated. His own subjects began looking to the future, when a new monarch would bring pride back to the throne and the United Kingdom, particularly after losing the American Revolutionary War. In fact, in the last ten years of his life, from 1810-1820, he was technically still king but his son, who would eventually succeed him as George IV, ran things due to George’s mental illness. But George IV wasn’t the future; his daughter was.
George IV’s only legitimate child was Princess Charlotte of Wales, born in 1796. She (or her children) were destined to inherit the throne. Since the monarch was both King of the United Kingdom and King of Hanover at the time, the people hoped that Charlotte would have a son, since Salic Law, which covered the Kingdom of Hanover, required a male to inherit. If a queen inherited, then the kingdoms would be split again. George IV wasn’t very popular either; he was a gluttonous, obese, alcoholic womanizer at his best. Like his father, he too lost a war to the US (the war of 1812). In the United Kingdom, public affections were directed towards the young Princess Charlotte, who was the only legitimate grandchild of George III at the time.
Charlotte eventually married a German prince called Leopold on May 2, 1816; Leopold would later become Leopold I, King of the Belgium. The two were widely celebrated and the young couple was adored by the public, in the same way that the marriage of Charles and Diana was celebrated in more recent times. The public hoped for a male heir to be produced by the union.
Charlotte quickly became pregnant and publicly acknowledged a miscarriage in 1816; some speculate she also had a second miscarriage. In July, 1817, it was announced that she was pregnant again and that she was expected to carry this pregnancy, due sometime in October of that year.
Charlotte had discussed with her friend, Lady Ashbrook, who should provide her prenatal care, and the women agreed upon Sir William Knighton. Unfortunately, the Queen made a different choice for Charlotte, and rather than Sir Knighton, a man called Sir Richard Croft was employed instead to attend to the Princess. Croft was known as the go-to obstetrician or accoucheur for the noble class, and decorum demanded that he be retained for the Princess rather than the perhaps more competent Knighton.
Croft’s care for her in the Fall consisted mostly of bed rest, dieting, and bleeding. Towards the end of the pregnancy, she had excessive weight gain and severe headaches, signs perhaps of “toxemia” or preeclampsia. These symptoms were met with more blood-letting to let out the toxins.
Her labor finally started with spontaneous rupture of membranes (SROM) at 42.1 weeks on Monday, November 3rd, 1817 at 7 pm. She was confined at Claremont House. Richard Croft was in attendance, and he called for back-up: his brother-in-law Matthew Baillie also was present. Baillie and Croft had married the twin daughters of Dr. Thomas Denman, a notable London Obstetrician who had written a textbook on the subject in 1788 and who had personally trained the two men.
Unfortunately for Charlotte, now post-dates and likely preeclamptic, she was not in labor when her water broke and initial progress was very slow. Her labor did start and she was noted to be complete at 9pm, November 4th, 26 hours after her membranes ruptured. Croft called for an operative obstetrician named John Sims, who arrived seven hours later (though he never examined the Princess). Some 15 hours after noting that she was completely dilated, the fluid turned to meconium-stained. Physicians of the time realized that this was an indicator of fetal distress.
Croft did not allow her to eat during her labor at all. A full 24 hours after becoming completely dilated – and 50 hours after her water initially broke – she finally delivered on November 5th at 9pm. A lifeless boy weighing 9 lbs (and who was later referred to as Harold because of Lord Byron’s poems) was born and futile attempts at resuscitation were made by Baillie and Sims in the adjoining room while Croft tended to the Princess.
The placenta was slow to separated and Croft performed manual extraction. She suffered a postpartum hemorrhage (PPH) and Croft left the placenta in the vagina to “tamponade” the bleeding. At about midnight, Princess Charlotte was suffering from nausea and vomiting and complained that she was hearing voices (delirium). She had chills and convulsions before becoming faint and quiet. She died at 2:30 am.
At post-mortem, she was discovered to have one pound of blood in her uterus. The infant appeared normal. They were buried together at Windsor Castle and a statue there shows Charlotte and Harold ascending into Heaven.

In the dust The Fair haired daughter of the Isle is laid,
The Love of millions, how we did entrust futurity to her.
– Lord Byron
The public was beside itself in mourning. The future of England had been lost. Many were quick to lay blame on Croft himself. A few months later, on February 13th, 1818, Croft was attending the birth of the wife of the Royal Chaplain, waiting in an adjoining room during a long labor much like Charlotte’s. Overcome with anxiety, he killed himself with a gun; next to his body was found a copy of Shakespeare’s Love’s Labor’s Lost turned to Act V, Scene II: “Fair Sir, God save you! Where is the Princess?”
Historians have called this the “triple obstetrical tragedy,” because the mother, infant, and obstetrician were all lost as a result.
George III was now left without a legitimate heir. Almost immediately, his surviving children who were able raced to produce a legitimate child. This almost three year period is British history is known as “the Baby Race.” Two of his sons abandoned their mistresses to take wives. Another bachelor quickly got married. The Duke of Clarence, the future King William IV, achieved a pregnancy first, but this was a premature child that died in 1819. This was followed by another 30 weeks loss. Prince Edward, the Duke of Kent, married Prince Leopold sister, Princess Victoria in 1818 and they had a girl in 1819 named Princess Alexandrina. George III died in 1820 and George IV became king until his death in 1830. William IV then reigned for 7 years until his death when finally Princess Alexandrine ascended to the throne at age 18, taking the name Queen Victoria in 1837.
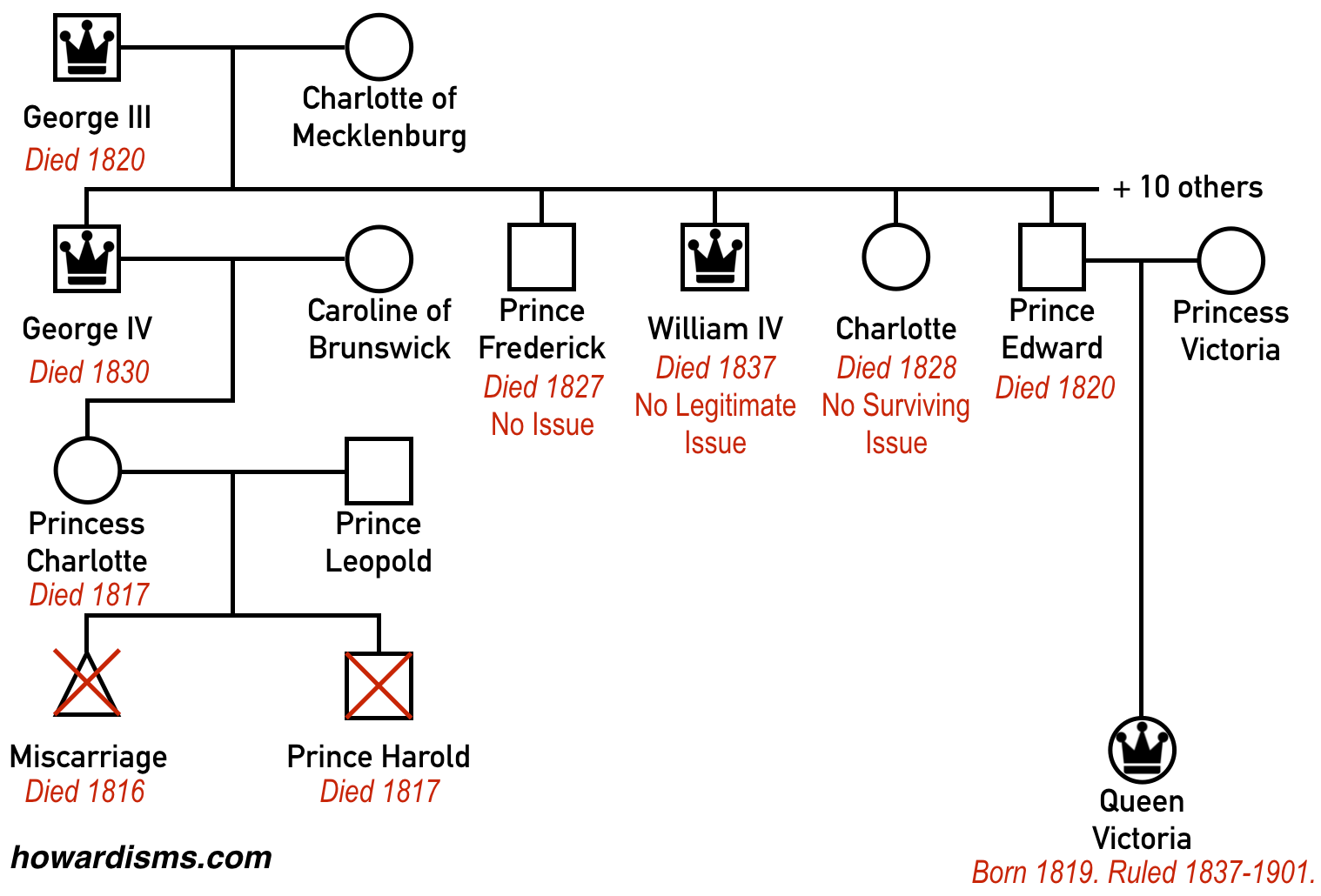
Victoria married her first cousin and there are some other interesting Obstetric stories to be told regarding her, but this Queen, who would have never been born if not for the deaths of Charlotte and Harold, changed European history. She reigned for 63 years and had six children. When she ascended to the throne, because she was female, the Kingdom of Hanover was separated from the United Kingdom. The royal families became divided and competitive. There was a resurgence in German nationalism and continental resentment. Eventually, a large family feud broke out between her grandchildren, including George V, King of the United Kingdom, Kaiser Wilhelm of Germany, and her first cousin Czar Nicholas of Russia who had married her granddaughter. This family feud was called World War 1, and it killed more than 70 million people. The unresolved issues of World War 1 then led to World War 2, claiming another 85 million people.
Am I claiming that an obstetric accident in 1817 eventually led to the death of over 155 million people? Well, I guess I sort of am. Who knows how European history might have played out had Harold been born alive and eventually ascended to the throne. Perhaps the unification of the royal families of the United Kingdom and the Kingdom of Hanover would have stabilized central Europe or perhaps Queen Charlotte would have been a much different ruler than Victoria, not only handling European events differently but also treating India differently. We will never know. One thing is for sure though: if Charlotte (and Harold) hadn’t died that night, Victoria would have never existed and the people in power at the turn of the 20th Century would have never been born.
So let’s examine what went wrong with Charlotte’s pregnancy by performing a root cause analysis.
Charlotte’s death. The cause of death can be debated, but given what we know, it seems likely that shock secondary to hypotension, sepsis, or both was the culprit. The large amount of blood in her uterus discovered postmortem would seem to indicate uterine atony as a causative factor. She may have been anemic before labor started secondary to the antenatal blood-letting. Her rigors and chills, combined with 50 hours of ruptured membranes, makes infection also likely. When Croft decided to leave the placenta in her vagina as a “tamponade,” this likely just concealed the outlet for blood loss, causing it be unrecognized and retained in the uterus itself. The attendants actually left her alone shortly after delivery thinking all was well, clearly not recognizing that hemorrhage was continuing.
The practice of leaving the placenta in the vagina as a tamponade in cases of hemorrhage was unorthodox even for the time, but had been championed by Croft’s and Baillie’s father-in-law, Thomas Denman, in an 1816 edition of his textbook. More about Denman momentarily.
Today, we prevent women from becoming septic by responding to premature rupture of membranes with induction of labor, chiefly with Pitocin. Had Pitocin been available to Charlotte, she would have likely delivered almost 30 hours earlier and sepsis averted. If sepsis or chorioamnionitis had been present, today we treat with antibiotics. She very well may have been Group B Strep (GBS) positive, and today we would have screened her and treated prophylactically.
The resultant postpartum hemorrhage was no doubt precipitated by a tired and worn out uterus. The principle treatment (and prevention) for uterine atony is, once again, Pitocin. If we use birth in Africa as a means of comparison, it is reasonable to assume that Pitocin saves the lives of hundreds of women each week in the United States by preventing or treating postpartum hemorrhage (PPH) due to uterine atony.
If Charlotte did indeed develop preeclampsia before her labor started, as evidenced by the swelling and headaches that led to Croft’s bleeding treatments, then this too would have been solved in modern Obstetrics by timely induction of labor when signs and symptoms first started. This induction of labor would have likely been facilitated by – you guessed it – Pitocin.
Harold’s death. We can’t know the exact cause of Harold’s death, but we do know that he passed meconium (and was therefore still alive and in distress) at least 9 hours before he was born. Worse, by the time he passed meconium, Charlotte had been completely dilated for 15 hours but remained undelivered. The passage of meconium was recognized at the time as a sign of fetal distress; still, even though Charlotte was completely dilated, nothing was done for a full 24 hours of complete dilation and 9 hours after the observation of meconium.
What could have been done at the time? Forceps. The Chamberlen family had been using forceps to deliver babies (albeit in secret) since at least 1634. The family secret found its way into a textbook of Obstetrics by 1735 and at the time that Charlotte was laboring, forceps were widely used in Obstetrical practice. In fact, few providers would have hesitated to use forceps in this delivery, given the circumstances. However, one textbooks of obstetrics went against the grain and recommended a strict conservatism in the use of forceps, including the criteria that the fetal head had to be crowning for six hours before they were applied. Can you imagine crowning for six hours? You guessed it: that controversial criterion was in Thomas Denman’s textbook, the father-in-law of Croft and Baillie. It is quite reasonable to assume that nearly any other Obstetrician of the day would have intervened sooner, perhaps making a difference. Recall that Sims, who was proficient with forceps, had been called to the delivery and was present for 17 hours before Harold was finally stillborn. But Croft, who wanted all the glory of delivering the future monarch to himself, never allowed Sims to even examine Charlotte.
Even without forceps, one would think that Pitocin might have made for more effective contractions, delivering the child much sooner. If Harold died of sepsis, then we can also safely assume that things might have been different if Pitocin was used at the first, after her water broke. Perhaps he was already dead, due to post-datism? Or would have succumbed to meconium-aspiration syndrome? Perhaps there had been a prolonged abruption? Today, we would have induced Charlotte 8 days before her water broke, at 41 weeks, specifically to prevent these tragic outcomes (and we would have used Pitocin).
Croft was a diffident rule-follower, who lacked ingenuity, creativity, vision, or the ability to think for himself. His biographers have described him as average and just not that smart. Louis Hellman said of him,
A lonely man in the delivery room upon which the eyes of the world were focused, he had neither the fortitude nor the imagination to defy established tenets.
The blood-letting, the placenta-tamponade, the nonuse of forceps, the lack of deference to Sims – all of these things no doubt contributed to the triple tragedy (and perhaps the quadruple tragedy if you buy the World Wars hypothesis). The worst part is that Charlotte herself never wanted Croft as her Obstetrician; recall, she wanted Sir William Knighton. Might he have avoided Croft’s mistakes? We can’t know for sure, but we do know that his father-in-law was not Thomas Denman.
So the root cause is picking the wrong Obstetrician. But think of how different the world might be had Pitocin existed at the time and Charlotte had had an Obstetrician willing to intervene when the circumstances dictated it instead of being a coward.
Since the time of Charlotte and Harold’s death, maternal and neonatal mortality has dropped more than 100-fold. Pitocin is a big reason for this. Just like forceps, it should only be applied when needed; but when needed, it is life-saving.
Source for more about Charlotte
Published Date : September 8, 2017
Categories : Cognitive Bias, Evidence Based Medicine, OB/Gyn

Physicians have a lot of power over patient choices. In theory, physicians present patients with choices and then patients make informed decisions. In practice, this almost never happens. A physician can manipulate a patient into doing almost anything by counseling patients in a biased and skewed way; a doctor may even tell the truth, but if the information is presented in a certain way, the patient almost always will make a certain choice – and this choice may not be the best choice for the patient.
Let’s consider the example of external cephalic version (ECV) for non-cephalic pregnancies. This practice is woefully under-utilized. ECV is not offered to everyone who is a candidate, but even when it is offered, women often don’t choose it. Why don’t they choose it? It’s all in the counseling. If the obstetrics provider doesn’t want to do it or has a negative opinion of the practice, it will be obvious in the counseling, which will focus on potential negatives and potential risk factors for failures, rather than potential positives and risk factors for success. We manifest what we focus on, and what we focus on is not necessarily based on scientific evidence. Performing ECV on all eligible patients is the right and evidence-based thing to do, but most providers don’t. Performing vaginal hysterectomy on all eligible patients is the right and evidence-based thing to do, but most providers don’t. Performing vaginal birth after Cesarean is the right and evidence-based thing to do, yet most providers don’t. I could go for hours. In all these cases, those average providers would say something like, “Well I offered it to her, but she chose the other option.” Yet, therein lies the rub: it’s all in the counseling. This biased counseling, designed to persuade but not to inform, is paternalistic medicine at its worst.
Imagine this conversation between an obstetric provider and her patient, who is a 37-weeks G1 with a breech baby:
Version is an option, but I’m hesitant because you have an anterior placenta. I don’t like to be too aggressive with anterior placentas. The small chance that it works and that you would go on to have a vaginal delivery isn’t worth the risk of an emergency Cesarean.
This type of counseling is just daring the patient to say no to ECV. It’s full of scary words like “aggressive” and “emergency” and uses qualitative and vague words like “small chance” rather than concrete and quantitative words. This is persuasion, not informed consent.
Consider some actual data points regarding ECV:
Now let’s examine the counseling in light of facts:
So here is a fairer statement to make to this patient:
If we do nothing, you are almost guaranteed to have a Cesarean delivery; this might be planned at 39 weeks or might be emergent if you present in labor before then. Either way, Cesarean delivery carries substantially higher risk for both the mother and baby, including a nearly 7-fold increased risk of maternal death. If you want more children in the future, each pregnancy will be riskier if you have a Cesarean compared to having a vaginal delivery in this pregnancy. Even though you have some factors which make an ECV harder to do, you still have about a 60% chance of success. There is a very small risk that something will happen at the time of the ECV that will require an emergency Cesarean delivery, but we will be in the hospital and ready for this. In fact, think of it this way: there is maybe a 1% chance that you will have to have an unplanned Cesarean at the time of ECV, but if do not attempt the ECV, there is almost a 100% chance you will have a Cesarean delivery, and because you may go into labor before 39 weeks, there is about a 10% chance that you will have to have an emergency Cesarean delivery if you don’t do the ECV.
Which provider sounds like she believes in evidence-based medicine and practices both competent and compassionate care? It’s all in the counseling.
We focus too much on worst case scenario thinking in medicine. Any potential scenario can be presented in three different ways: describing what might happen in the worst case scenario, what might happen in the best case scenario, and what typically happens in most scenarios.
What if the hypothetical bad doctor above were to counsel a mom about taking her two young children to the park to play? How would she counsel her if she were consistent in style?
You should know that going to the park involves driving a car; there have been situations where even perfect drivers were struck by other cars and killed. In fact, you and your children could be killed or suffer other injuries that would leave you or your children permanently disabled. Even if you do nothing wrong, your car might suffer mechanical failure that causes you to crash, potentially killing you or others. If you are fortunate enough to make it to the park, there are dozens of dangers awaiting, including kidnapping, broken bones, etc. I think if it were me, I would just stay home and watch TV. After all, better safe than sorry. I just want a healthy momma and healthy babies.
This is worst case scenario thinking, and doctors are plagued by it. Of course, the average scenario is that they go to the park and have a good time. The best case scenario is that they go to the park, stop for gas, by a lottery ticket, and become millionaires. It is just as legitimate to go through this best case scenario as it is the worst case scenario. What patients need to know is what typically happens and how to avoid unnecessary risks. Yes, you and the kids should buckle up while going to the park (do the ECV in the hospital) and you should keep an eye on the kids (monitor the baby before, during, and after the ECV), but overall, the benefits of going to the park outweigh the risks.
When I first wrote the hypothetical counseling paragraph about going to the park, it was much more gruesome; my editor told me it was too much, too graphic, and sickening to think of what could happen to small children. She felt it was gratuitous. So I softened it and took out some of the graphic descriptors. But that is the point: no mother can stand to think of something bad happening to her child, whether at birth or going to the park. I can tell the truth about possibilities and use the right filter and tone and manipulate any mother into doing anything. My editor couldn’t even finish reading it, thinking about the horrors being described about young children, and that wasn’t even a real scenario. In the same way, no reasonable mother would ever choose ECV (or VBAC, etc.) with this type of worst case scenario description. Physicians have no right to prey on the fear of mothers.
It is all in the counseling. If you want to scare someone into not doing something, give them the worst case scenario. If you want to talk someone into doing something, give them the best case scenario. If you want to counsel someone in an ethical and compassionate way, give them the average and expected scenario along with a quantified and balanced assessment of both risks and benefits. It’s their decision, not yours.
Published Date : August 16, 2017
Categories : #FourTips
One of the obvious benefits of a laparoscopic surgical approach compared to an open approach is less pain and morbidity related to smaller incisions and less wound morbidity. Postoperative pain in general is reduced with laparoscopic surgeries, but a unique type of pain is found in up to 80% of surgeries: post-laparoscopic shoulder pain (PLSP), which is thought to be related to residual carbon dioxide causing diaphragmatic irritation of the phrenic nerve, as well as phrenic nerve neuropraxia. This type of pain doesn’t respond to pain medications as well as pain that is related to the incisions or the surgery itself does. Clearly, not all laparoscopic surgeries are created equal and levels of postoperative pain vary widely. Here are four tips to reduce postoperative pain related specifically to laparoscopic surgery.
1. Get the gas out.
Since there appears to be a relationship between the residual amount of gas and PLSP, then getting all the gas out would seem to be important. At a minimum, you should allow the capnoperitoneum to drain from an open, distal trocar (the lowest one) while applying gentle abdominal pressure. But better than that is to use the pulmonary recruitment maneuver (PRM). To do this, place the patient in 30° of Trendelenburg while opening the most distal trocars (this encourages the gas to rise to the lower abdomen); then have the anesthesia provider provide five manual pulmonary inflations up to 60 cm H20. Have the anesthetist hold the last inflation for five seconds. This maneuver increases the intra-abdominal pressure. Then flatten the patient and remove the trocar. This simple step has been shown to reduce PLSP-type pain from 64% to 31% and also reduce postoperative nausea or vomiting from 56.5% to 20.4%. It also reduced the need for postoperative pain medication. A recent study has shown that this maneuver works just as well even if the inflation pressure is only 40 cm H20.
2. Make smaller holes (but not necessarily fewer).
This sounds intuitive; one of the obvious advantages of doing a case endoscopically compared to doing it through a laparotomy is the smaller incisions. But remember, the smaller the better. If you can use a 5mm trocar, you’ll have less pain than if you use a 10 mm trocar. Modern instrumentation and optics has made larger trocars all but unnecessary. However, reducing the number of incisions by converting to single-port access laparoscopy doesn’t help reduce pain. Most gynecologic cases can be completed easily with two or three 5-mm trocars. Some diagnostic laparoscopies need only one 5 mm umbilical trocar. Almost all gynecologic surgeries can be performed through a single umbilical port as well, including hysterectomies, but that single port is usually about 18-mm. But don’t fall for the hype. Evidence shows that single-incision surgeries provide no advantage and take longer, but they don’t reduce pain and they are associated with higher risks of herniation through the larger umbilical incision.
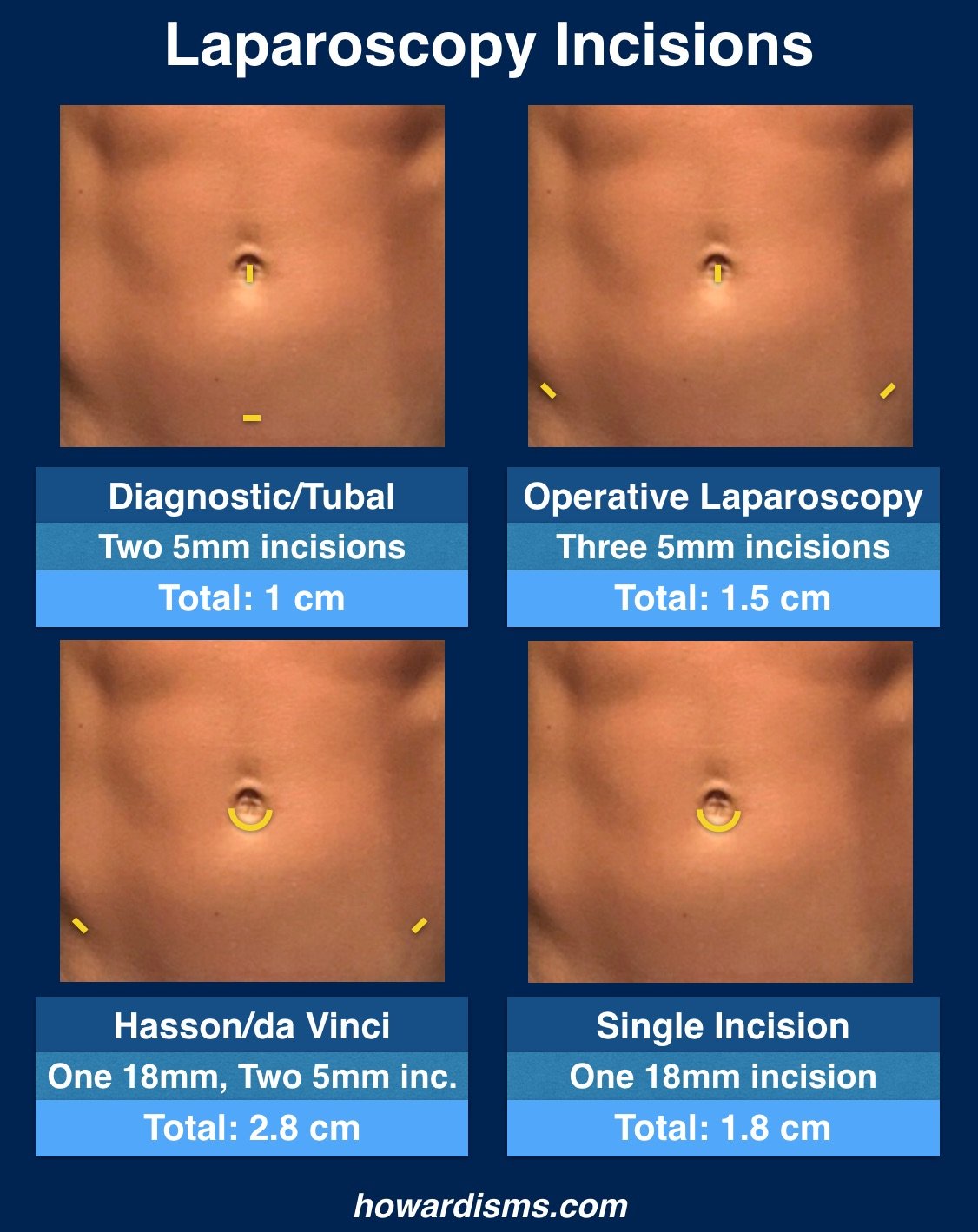
Of course, if you are performing open laparoscopy with a Hasson cannula, you are probably already making a 15 to 18-mm hole and single incision surgery might provide an advantage. But you should be using a 5 mm direct entry trocar in the umbilicus and replacing this small incision with a larger incision is associated with more pain and hernianation risk.
By the way, if you perform sterilizations with a Filshie clip applicator, you don’t need an 8-mm or 10-mm port to insert the loaded application; a 5-mm trocar works just fine.
3. Stop using so many uterine manipulators.
Traditionally, some sort of uterine manipulator is used with most gynecologic laparoscopies if the patient still has her uterus. Many of these manipulators require cervical dilation and instrumentation of the uterus. But they are rarely necessary. Most tubal ligations, salpingectomies, oophorectomies, and diagnostic laparoscopies can easily be done without a uterine manipulator. If you know specifically that you are a doing a procedure that involves the posterior cul-de-sac (more than just looking at it) or a uteropexy procedure or other complex surgery that requires specific uterine positioning, then a uterine manipulator can be very useful. A uterine manipulator is also very useful for ruptured ectopic pregnancies, where elevating the uterus up and out the cul-de-sac (along with steep Trendelenburg) can allow for rapid visualization of the rupture tube. Otherwise a sponge-stick placed in the vagina serves most purposes and your patient will not have to experience the pain of having her cervix dilated and her uterus instrumented unnecessarily.
4. Give perioperative ketorolac.
A single perioperative dose of ketorolac (60 mg) reduces postoperative pain in the first four hours after surgery, reduces postoperative nausea and vomiting by half, and shortens the time to discharge. Unfortunately, many surgeons are hesitant to use perioperative ketorolac due to an unfounded fear of bleeding. Rest assured, this concern about bleeding is completely unscientific.
What else?
Don’t inject local anesthetic at the trocar insertion sites to reduce pain; this strategy, used by lots of surgeons, has been studied extensively and doesn’t work.
Using 5-mm trocar means you don’t have to close the fascia with suture, which reduces foreign-body inflammation and associated pain.
You also don’t need to close the skin with suture; Dermabond or a similar adhesive is an excellent alternative and saves times and money. Reduced time of surgery will also reduce postoperative pain.
Lastly, try to keep your insufflation pressure as low as you can, under 15 mm HG if possible. This is also associated with less pain.
Published Date : August 1, 2017
Categories : #FourTips, OB/Gyn
Unfortunately, I’ve recently seen a rash of patients who have been told by other gynecologists that they suffer from a significant congenital uterine malformation that will require extensive workup, probable surgery, and will significantly hinder their ability to reproduce. Yet, in each case, the women either had no uterine abnormality at all or a mild arcuate appearance of the uterus – despite being informed that they had a didelphic or deep septate uterus. What I’ve noticed in each case is that the original gynecologist didn’t understand the basic nomenclature used to describe Müllerian anomalies and they certainly did not understand how to interpret the ultrasound findings correctly, since in each case the women were to be referred for an MRI as a first step in additional evaluation. The wasted cost and mental anguish expended upon these patients was completely unnecessary. So here are four tips for correctly diagnosing uterine anomalies with ultrasound to try to prevent these common mistakes.
1. Know the embryology and nomenclature well.
People hate to think about embryology, but understanding the embryology of the uterus is essential to correctly understanding the different types of uterine anomalies and how to diagnose them. Too often, physicians will refer to any uterine anomaly with a broad term like bicornuate uterus due to a lack of understanding of the terminology. So let’s have a brief review.
The uterus, fallopian tubes, and the upper two-thirds of the vagina arise from the bilateral Müllerian ducts (or paramesonephric ducts) after sexual differentiation and regression of the Wolffian ducts. Problems may arise from the failure of either or both ducts to form or form completely. The lower third of the vagina develops from the ascending sinovaginal bulb, which must eventually fuse with the developed Müllerian system.
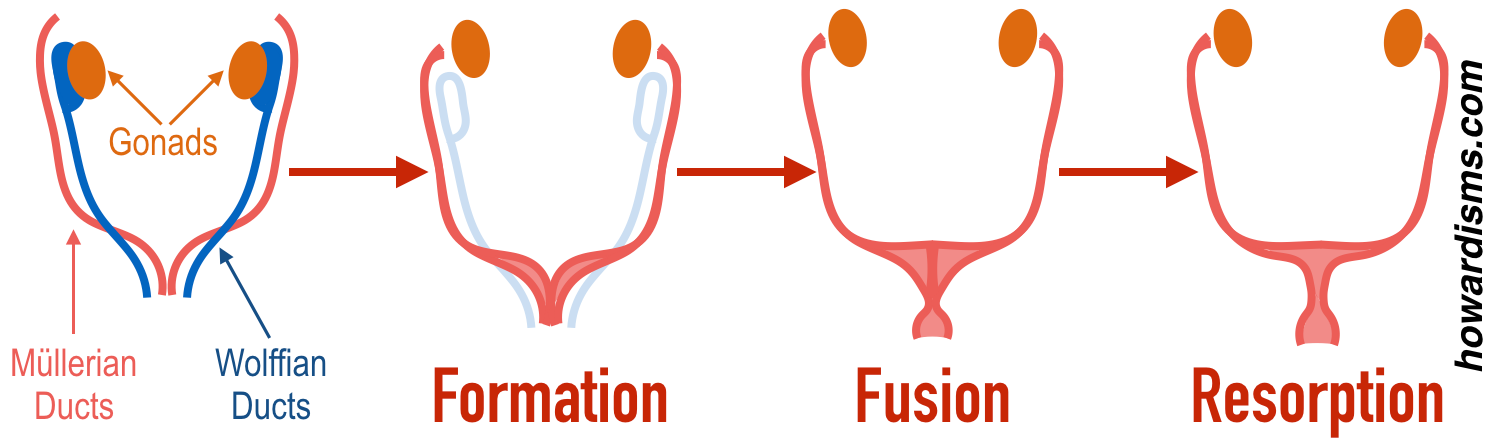
These structures must all completely form, fuse together, and, finally, the horizontal and vertical septa created during fusion must resorb to have normal female anatomy.
Therefore, abnormalities may develop from a lack of development (agenesis or hypoplasia), a problem with fusion, or a problem with septal resorption.

2. Define the external contour of the fundus.
When any woman has an ultrasound of the uterus, always scan completely through the sagittal view of the uterus, following the contour of the fundus, to see if there is an abnormality.
Recall the anatomic planes:
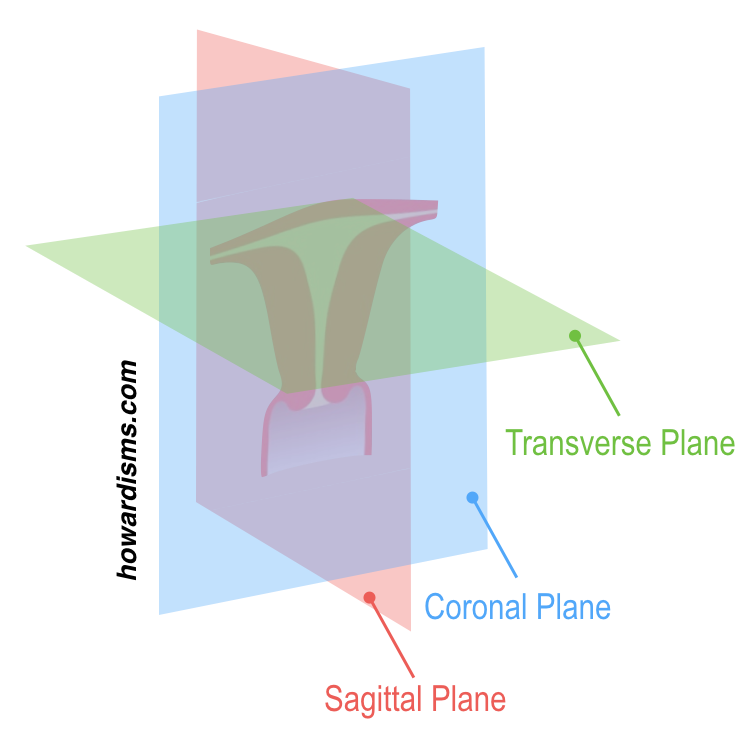
This means that the sagittal plane of the uterus looks like this:
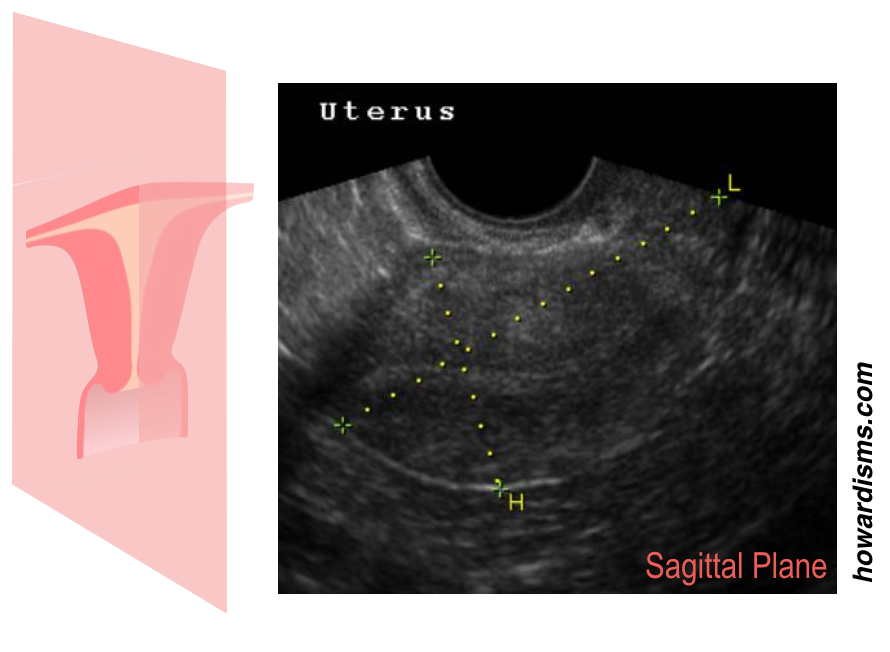
By scanning from one cornua to the other and watching the top of the uterus, abnormalities related to incomplete fusion (like a bicornuate or uterine didelphys) can be detected. This view is always easy to obtain with transvaginal ultrasound.
3. Compare the fundal myometrial thickness to the corneal myometrial thickness.
While looking at the external contour of the uterus, also note the thickness of the fundal myometrium in two places: near the cornua and in the center of the fundus. If there is a concern about an abnormality, then the thickness of the myometrium can be measured near the cornua (Tc) and also measured at the center of the fundus, at its thickest point (Tf). The difference in these two measurements (Tf-Tc) approximates the size of internal indentation of the uterine cavity which might represent an arcuate or septate uterus.
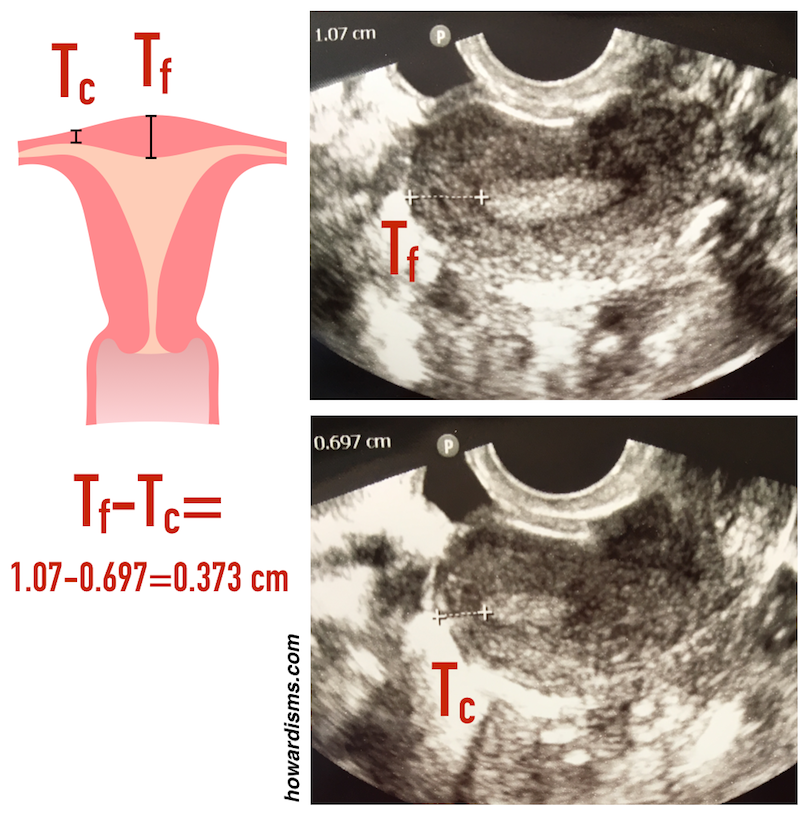
In this case, the difference is 3.7 mm, which is not clinically significant but can make the uterus look concerning when the endometrium is viewed in a transverse plane:
![]()
The endometrium is divided by the small internal indentation of the myometrium, giving a “cat’s eyes” sign. This patient was told that she had a Müllerian abnormality (a septate uterus) based on this ultrasound view and was told she would likely need surgery to correct it. Yet, the same conventional ultrasound, in a universally obtainable sagittal plane, shows only a 3.7 mm indentation, which doesn’t even qualify it as arcuate by modern criteria. Many thought-leaders are moving to remove the classification of arcuate uterus from the nomenclature entirely since this common finding has little to no impact on reproduction.
Müllerian abnormalities can affect fertility in two primary ways: an increased risk of miscarriage and/or an increased risk of preterm birth. Miscarriage risk is increased in cases where some of the surface area of the uterine cavity is replaced with septal tissue, which is less vascular and therefore less able to sustain an implanted pregnancy than normal myometrial tissue. Therefore, uterine anomalies due to incomplete resorption are associated with an increased risk of miscarriage.
Preterm birth is increased if the size of the cavity of the uterus is diminished or constricted. Uterine hypoplasia or unicornuate, bicornuate, or didelphic uteri are all associated with a physically smaller cavity and therefore an increased risk of preterm birth.
A uterus with both diminished cavity size and an increased avascular surface area, such a complete septate uterus, would increase the risk of both miscarriage and preterm labor. Fortunately, septate uteri are often candidates for septoplasty and this surgery can improve pregnancy outcomes.
The following algorithm can be implemented with conventional transvaginal ultrasound in most patients, simply by examining the external contour of the uterus (looking for a cleft) and assessing the internal cavity as described above:
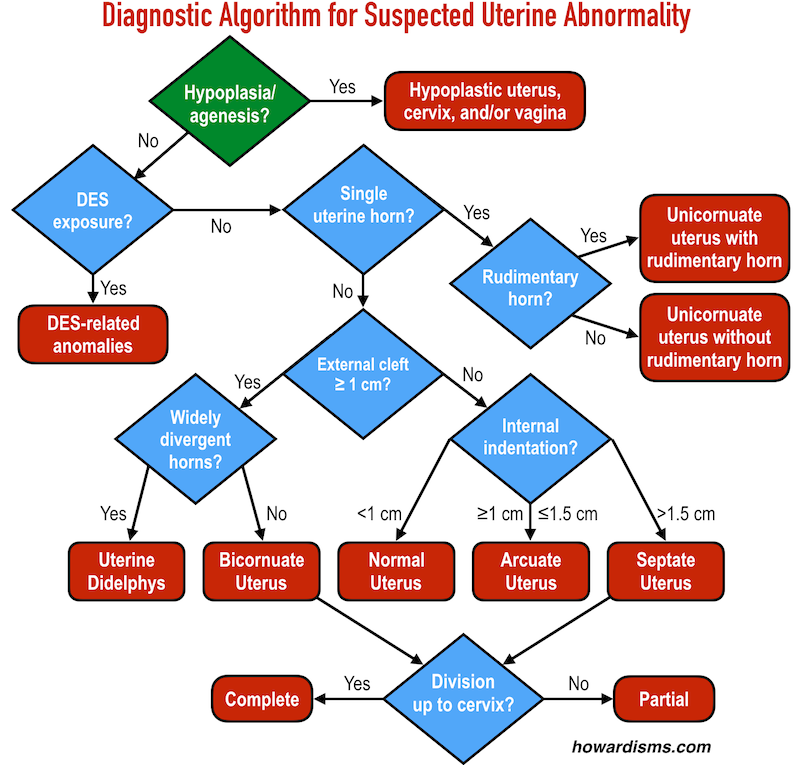
4. Use saline infusion, 3D ultrasound.
In some cases, traditional 2D ultrasound is insufficient to definitively determine the nature of the uterine malformation. It is usually very difficult to get a true coronal view of the uterus, which would be most helpful for assessing a deep septum or a deep cleft. If there is a suspected cleft or a deep septum, then 3D ultrasound, with or without saline infusion, can be diagnostic, and is less expensive and more accessible than MRI.
Here is a coronal view of a complete septate uterus reconstructed using 3D ultrasound:
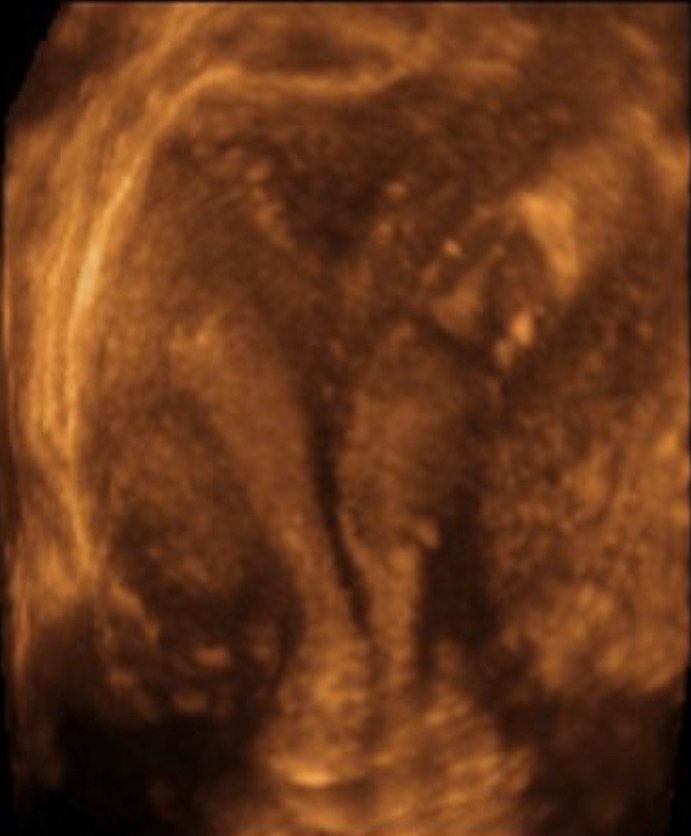
Note that there is no cleft along the top of the fundus, indicating complete fusion, but a septum that extends all the way through the cervix, indicating a complete lack of resorption. The addition of saline infusion can further enhance this type of study.
MRI may still be necessary to discover a rudimentary horn or other unusual anomalies, but these are not usually clinically relevant and often don’t inform the counseling of women regarding their reproductive options and outcomes.
What else?
Don’t scare patients with misinformation. There just is no clinical relevance to mild fundal indentations or even arcuate uteri. These are essentially normal variants.
Examine the vagina well. A careful exam of the vagina and cervix may reveal vaginal septa or other abnormalities. It’s amazing how often women go many years not knowing that they have a vaginal septum or even two cervices!
Check out my video on Müllerian abnormalities for more information:
Published Date : July 24, 2017
Categories : Diet

When I talk to patients about weight loss, they usually tell me about their plans to exercise more and eat healthier. Recently, they ask me how I have lost 40 pounds or what magic I used to slim down. Most are sad to learn that there is no magic bullet. That being said, losing weight is rather easy and follows a set and predictable formula. In my case, as an insulin-dependent diabetic, the biggest difficulty was balancing blood sugars while losing weight. I’ll tell you what I did in a minute. But first, I would like to address those two keys I always hear people talk about: exercising and eating healthier.
Exercise definitely helps, but not in the way that one might anticipate. Exercise is helpful only in that it uses calories, but moderate exercise like walking burns few calories over the baseline metabolic rate, which means that walking adds next to nothing in terms of weight loss, particularly if a person adds a snack or a caloric exercise drink into the regimen. I have seen folks at the gym who are drinking a Gatorade or other “exercise drink” which contains more calories than the exercise they are doing consumes; these folks are actually gaining weight by going to the gym. You need real cardio to lose weight in a meaningful way: running, swimming, rowing, biking, chopping wood, etc.
“Eating healthier” is a vacuous and imprecise statement. I have talked about some of the myths related to dieting here, but suffice it to say that the only healthy thing one can do to lose weight in terms of diet is to eat less food. There are no superfoods, detoxes, metabolism-boosters, or diet plans that help a person lose weight; you just have to eat less. Understanding the caloric density of foods is important and can help you cut calories, but switching one type of food for another or restricting certain macronutrients like carbs or fats, unless it leads to fewer calories, won’t help you lose weight.
As much as people hate it, weight loss really is just about using more calories than you take in. You can do only two things: eat less and do more. Do both of these things and you’ll lose weight more quickly than if you do just one. But nothing else matters. Period. If you are honest about how many calories you take in (which can be very difficult), then your weight will follow a very predictable pattern. If you feel like you aren’t losing weight on your diet, it is simply because you are eating too much. Every obese patient I have ever met tells me that they don’t eat that much, but I can calculate how much they are eating by knowing their weight and activity levels. It may not seem like they are eating a lot to them, but they are still eating too much to lose weight.
Let’s look at what I did:
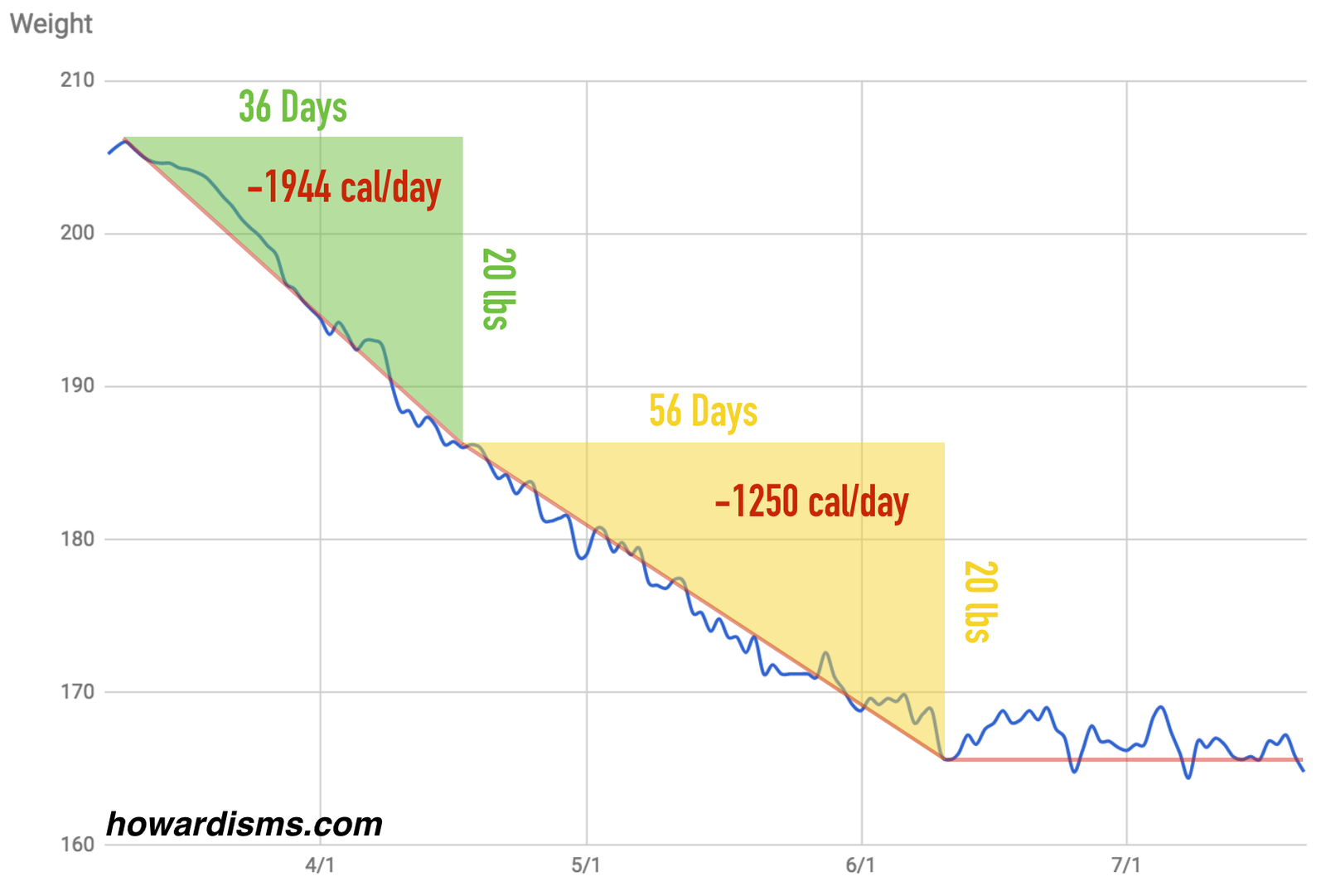
I lost 40 lbs between about March 10th and June 10th. The first 20 lbs took 36 days and the next 20 lbs took 56 days. Since then, my weight has fluctuated around 166 lbs (I started at 206), running between 164 and 169 lbs. Since one pound of fat is roughly equivalent to 3500 calories, then this means that I had to run a caloric deficit of 140,000 calories over those 92 days (about 1,000 Twinkies). As the graph above shows, I lost weight more quickly at first, averaging an almost 2000 calorie deficit each day, and then slowed down, but still averaged about a 1250 calorie deficit each day. Why the difference? Because I ate more and did less during the second 20 lbs lost than during the first. Here is a breakdown:

My caloric deficit is simply how many calories I used minus how many calories I consumed. The difference results in weight loss. Calories used is equal to the basal metabolic rate, which varies according to your current weight and gender, plus calories used with activity. As you lose weight, your caloric needs will naturally decrease (because you are smaller and are using less calories) and, therefore, you will either have to restrict even more calories to lose weight at the same pace, or just lose weight more slowly like I did. In the graph above, the blue line represents how many calories a man my size would need if he had a sedentary lifestyle; at 206 lbs, a sedentary male would require 2179 calories to maintain his weight while at 166 lbs, he would require 1961 calories (the blue line). Throw in some light exercise (20 minutes of cardio 3-4 times per week) and those numbers go up to 2497 and 2247 calories, respectively (the red line). If I were willing to do cardio every day of the week for 30 minutes, then my caloric needs would increase to 3133 and 2820 calories, respectively (the yellow line).
What I actually did at the gym is more represented by the purple line. I went intensely at first and my body was deconditioned so I used the most calories; later, I did less cardio and more weights and I was more conditioned, therefore using fewer calories. That’s the first thing we have control over: how many calories we use each day. The second part is how many we calories we consume.
I initially limited my daily caloric intake to 800 calories per day. By the second phase, I was eating closer to 1000 calories per day (the green line). The difference between the purple and the green line is my caloric deficit, and it very predictably resulted in the observed amount of weight loss.
I am sure I lost more than 40 lbs of fat, as I undoubtedly gained muscle mass. I lost 5 inches off my waste and got my 1-mile-run time down from over 13 minutes to under 8 minutes. I went from being able to do no pull-ups to being able to do more than 10. My BMI went from 31 to 25. Exercise has benefits far beyond weight loss, and truthfully, I don’t exercise enough. But as far as weight loss is concerned, it really is just a simple mathematical formula.
You can calculate your own caloric needs with this calculator. For many people who try to lose weight, the first round of dieting or calorie counting just gets them back to baseline. You don’t get obese by eating the right amount of food each day. If you are a sedentary woman who weighs 200 lbs, you can eat about 2,000 calories per day and maintain your current weight. But, the truth is, if you have decided to lose weight, it is probably because you have been gaining weight recently. If you’ve gained 20 lbs in the last 6 months, then you are not just eating 2000 calories per day. You are likely eating closer to 2500 calories per day. So when you start dieting, cutting 500 calories seems like a lot, but that was just enough to get you back to baseline. If you want to lose weight, you have to cut even more. If you wanted to lose the 20 lbs over the next 6 months, then you would have to cut 1000 calories per day from what you are currently eating (2500 minus 500 extra minus 500 to lose equals 1500 calories). Going from 2500 to 1500 calories seems drastic; but, this drastic cut will only result in losing about 3 lbs per month. This is why people quit their diets: because the drastic caloric cuts don’t seem to pay off in short term, recognizable results.
The psychology of eating so little is difficult. I believe that losing weight quickly helps, so that you can see the results and be encouraged by them. Severe calorie restriction also becomes easier with time because you become used to less food. For this reason, instead of focusing on feeling “full” by trying to eat large quantities of low calorie food, just eat less and adjust. There are no tricks, just discipline.
What is most eye-opening for people is the calorie content of the foods that they eat and how little they should be eating to lose weight. We misjudge portion sizes and misjudge calorie contents of food by a significant amount. Let’s look at some examples.
Remember, I was eating only 800-1000 calories per day (not per meal). I did this by skipping breakfast (yes, it’s the right thing to do according to science) and then allowing myself about 400 calories for lunch and 400 calories for dinner. When I went to 1000 calories per day, this allowed me a couple of 100 calorie snacks each day. To do this meant a few rules:
The other thing I had to do was reduce the amount of insulin I was taking, and I did so rather dramatically. I was often forced to “cheat” on my diet due to hypoglycemia, and I was surprised at how much insulin I cut out.
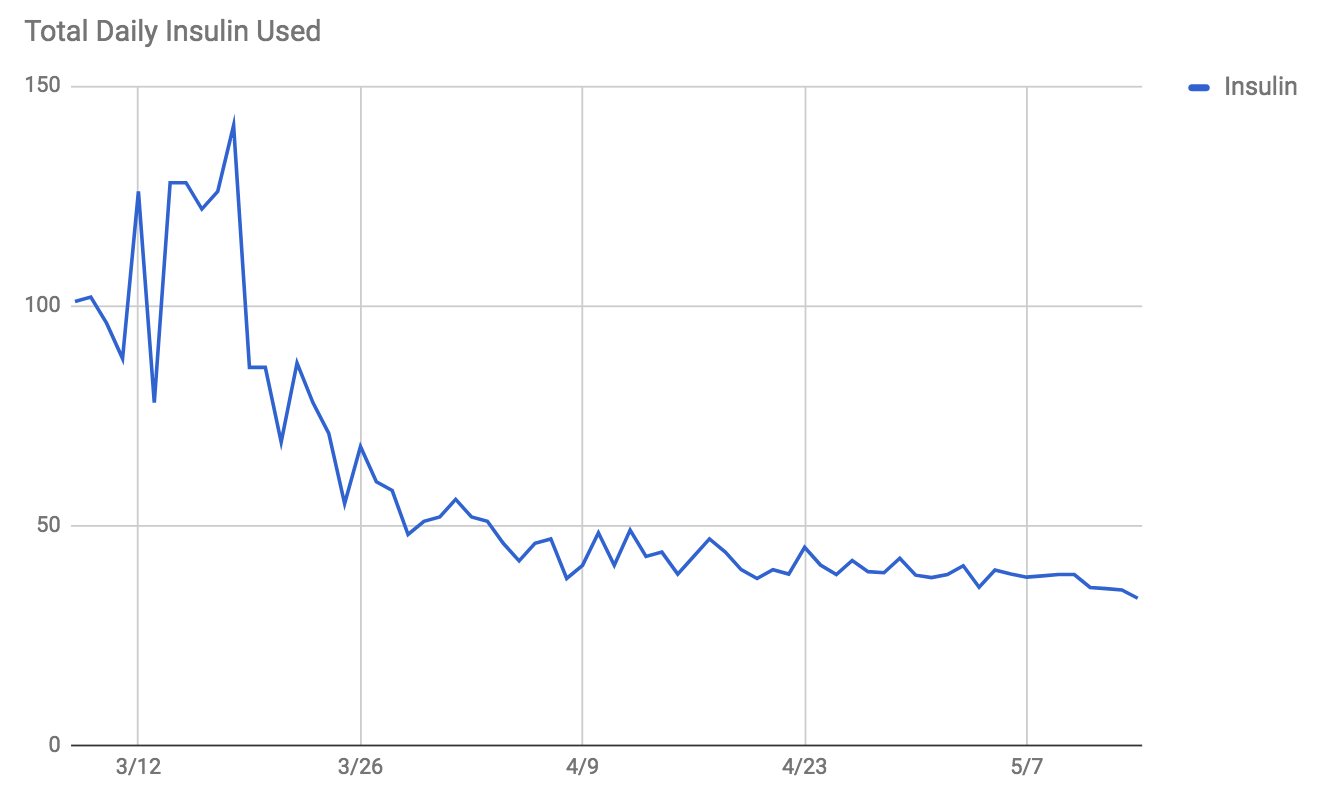
I went from an average of around 120 units of insulin per day to an average of around 40 units per day. Obviously, my blood sugar control improved as well with weight loss and caloric restriction.
One last point: I wasn’t that overweight or that out of shape when I decided to do this, but I was technically obese and sluggish. By lowering my weight and adding moderate exercise, I likely added about 5 years to my life expectancy, not including the positive effects on diabetes. Plus, my quality of life will be better for any remaining years. With the impact of better blood sugar control and exercise on diabetes, the true life expectancy addition may be in the 10-15 year range. Not bad for three months worth of work. Now imagine how much a more obese person has to gain!

Published Date : July 17, 2017
Categories : Evidence Based Medicine, OB/Gyn

I haven’t used a left lateral tilt during Cesarean delivery in years. There has never been any robust scientific data that tilting the table or tilting the mother with a rolled blanket or pillow to approximately 15° has any effect on fetal outcomes. Still, the practice is widespread and most practitioners believe it be of value. It has been included in many practice standards, albeit without evidence. But finally, a randomized controlled trial was published last month which analyzed this practice. The authors found no differences in fetal base excess or pH between the women who were tilted and those not tilted. Studies over the years have shown an increase in maternal cardiac venous return, but this surrogate maker has simply never been shown to translate into fetal benefit. We must be careful creating false de facto standards of care without evidence. The lateral tilt should be abandoned until fetal benefit is demonstrated.
Hopefully you already don’t make a bladder flap at the time of Cesarean delivery. The routine creation of a bladder flap lengthens the time of surgery, the time from start to delivery of the baby, and doesn’t decrease the risk of bladder injury or other complications. This archaic practice dates back to a time before antibiotics, and was originally intended to help create a retroperitoneal tunnel that would aid in isolation of vaginal flora from spreading around the peritoneal cavity, or to at least create a surgical flap that could be repaired over the uterine incision to make it and any potential leakage from the uterus retroperitonealized. This approach was made popular and dogmatized by Krönig in the early 20th Century, and worked best with a classical uterine incision (which would lie perpendicular to the peritoneal incision). The bladder flap was never shown to facilitate protection of the bladder from injury, and may, in fact, make injury more likely to occur by encouraging surgeons to make the hysterotomy too low in cases of deep arrest by removing and distorting visual landmarks. Now, a new study from 2017 also shows that women who receive a bladder flap report higher rates of urinary bother symptoms at 6-8 weeks postpartum, placing yet another nail in the coffin. There just is no reason to make one; stop doing it!
A lot of dogma surrounds the practice of amniotomy during labor. Clinical studies are contradictory about the benefits and risks of rupturing membranes, with some showing shorter labors but with higher rates of infection and others showing no benefits. Well-controlled studies have been lacking for decades. The result is that some obstetricians swear by amniotomy while others ridicule it.
A new study which will be published next month randomized 288 women in spontaneous labor to amniotomy or no amniotomy between 3-5 cm dilation, while controlling for other variables. The women with ruptured membranes had an average labor of 235 minutes compared to 364 minutes for the women who did not get their membranes ruptured, a difference of just over two hours. The Cesarean delivery rate in the amniotomy group was 2.8% compared to 6.2% in the control group, though the study wasn’t powered sufficiently to declare this statistically significant. This is not the first well-designed study to show a difference. Here’s one from 1993, which also showed 2 hours+ shorter labors with amniotomy. The well-designed studies are consistent in this finding. Amniotomy may not reduce the rate of Cesarean delivery, but it does make labor faster, and some women may find that appealing.
A 2014 study in the Gray Journal by Marrs et al. compared a transverse skin incision to a vertical skin incision at the time of Cesarean delivery. Surprisingly, they concluded that the odds of wound complications were lower among women with a vertical skin incision after performing a multivariate analysis. This didn’t quite make sense: in the univariate analysis, the risk of wound complications was lower in women with a transverse incision and this idea was in keeping with most of the rest of the literature in this regard. Fortunately, I wasn’t the only one who thought this study was flawed. Thankfully, it was retracted this month after it was discovered that an error was made in the multivariate analysis. It actually concluded the opposite of what was published. The transverse incision is indeed the safer choice for obese women.
It has been commonly rumored through marketing efforts that the larger umbilical incisions associated with single-port laparoscopic surgery do not lead to a higher rate of incisional hernias compared to the smaller, 5 mm umbilical incisions associated with traditional multi-port laparoscopic surgery. This counter-intuitive finding is based on weak evidence which has been augmented through the marketing departments of a myriad of companies involved in selling the expensive equipment needed for single-incision surgery.
However, a new review published last month shows that the intuition that a bigger incision leads to more hernias is correct. Among 908 women undergoing single-incision gynecologic surgery (mostly hysterectomy), 5.5% eventually developed an incisional hernia. The rate was as high as 23% among high-risk groups (women with obesity, diabetes, or hypertension). Interestingly, the timing of hernia development was an average of 570 days, which shows why shorter-term studies often fail to detect the increased risk of herniation, since most only follow the patients for a few months. The rate of hernia with traditional laparoscopic gynecologic surgery is thought to be far less than 1% (about 21 per 100,000).
A 2016 study examined the relationship between cervical dilation at the time of admission for labor and the Cesarean delivery rate among nulliparous women. Patients who were admitted in labor and were less than 4 cm dilated had a significantly higher risk of eventual Cesarean delivery (18% vs 4%) compared to women who were more dilated. This data is consistent with studies which previously examined active labor management (the Dublin method), where women were not offered admission for labor unless they were at least 4 cm dilated. Too often, women in early latent labor are admitted and then augmented with resultant labor dystocia. A woman who presents and changes from, say, 2 to 3 cm may not progress beyond that dilation for some time; she is likely not yet in active labor. Admitting her too early and then augmenting her when she fails to progress may quadruple her risk of a primary Cesarean delivery.
This same observation was made among multiparous women in another 2016 study. In this case, multiparous women admitted before 6 cm dilation had an 11% chance of eventual Cesarean delivery compared to women admitted at 6 cm or more who had only a 2.5% risk of eventual Cesarean delivery. A multiparous woman who presents at 4-5 cm and contracting regularly is often admitted without evidence of cervical change and assumed to be in active labor, though she too may still be in latent labor or not in labor at all. The concept that 4 cm equals active labor must be thoroughly rooted out of obstetrical thinking and management protocols. A 2016 Canadian review of indications for Cesarean delivery among 392,025 nulliparous women found that among those who underwent Cesarean for labor dystocia, 13.6% were less than 4 cm dilated and 29.5% did not receive oxytocin to treat the dystocia prior to undergoing Cesarean delivery. About 1 in 4 women were 6 cm dilated or less, and therefore not in active labor by today’s standards. We have to shift our mindset completely about the definition of active labor.
There are a lot of anecdotes (aka myths) that pervade Obstetric practice and thought. Be careful how your advice can cause these myths to persist. For example, if a miserable 40-weeks pregnant woman asks what she can do to help her go into labor, her doc might say something like, “Go home and have sex.” Since semen contains prostaglandins, and since we use prostaglandins to induce labor, many people believe that there is some value in sex in stimulating labor, even though there has never been evidence of this. Thankfully, there is now a randomized controlled trial from 2014 which analyzed this question. The authors found no difference in timing of delivery, vaginal delivery rate, or rate of spontaneous delivery when subjects were randomized to sex or no sex. Sex is fun (citation needed?), but it doesn’t put a woman into labor. When this myth is perpetuated, it makes women scared to have sex earlier in pregnancy and in some cases makes women feel guilty who have had a miscarriage or a preterm birth, feeling that they are somehow responsible for the outcome because they had sex.
Published Date : July 11, 2017
Categories : Cognitive Bias

Did you see all the fuss about the recent Amelia Earhart documentary on the History Channel? A picture, found in the National Archives, purportedly shows Earhart and her navigator, Fred Noonan, sitting on a dock at Jaluit Atoll in the Marshall Islands with their plane sitting on a barge in the distance. This photo, which would have been taken after the crash, is used in the documentary to argue that the two survived the crash, were captured by the Japanese, imprisoned by them while the US Government performed a cover-up, and eventually they died or were killed in prison.
This picture and the story was investigated with the latest scientific techniques by a former Assistant Director of the FBI. The latest in facial and body recognition techniques were used to positively identify both Earhart and Noonan, and the photograph itself was authenticated as having been unaltered with impressive forensic techniques. Even the airplane spotted in the background is an exact physical match for the Lockheed Model 10 Electra that Earhart was flying.
The documentary is very convincing and brings to bear the latest scientific evidence and investigative methods by leading experts to show what might have really happened to Earhart, and the newly discovered photograph is the key that has unlocked the mystery. Every major news network and US newspaper has covered this exciting new development and the implications of the bombshell new finding.
There’s just one problem: it isn’t true; the photo has nothing to do with Earhart, Noonan, or their plane, and it was already in print at least two years before they disappeared in 1937. It took Kota Yamano less than thirty minutes to find the source of the photograph online (yet somehow the highly-trained experts and former FBI agents investigating it for months fell for the fake photo). Here is the photograph in a Japanese travel book published in 1935:

So what lessons can we learn from this ridiculous mistake, other than that the History Channel stopped being a source of quality programming a long time ago?
Experts are wrong all the time. The parade of world-class experts who opined about the photograph were all brazenly wrong; as experts, they have too much faith in their techniques and too little skepticism. Experts disagree with one another all the time in every field, so it follows than most experts are wrong most of the time about most things. An expert is only as good as the evidence he cites, and you should never take the word of an expert; that is a logical fallacy called an appeal to authority. Assess the evidence they present and assess the evidence independently; it is the evidence that matters. The Japanese blogger who showed that the photo was a fake doesn’t have any of the “expertise” claimed by the men in the documentary, but he was right and they were wrong. Don’t over-value scientific studies because they were performed at a leading university or by a leading personality; assess the evidence independently.
Reporters who cover stories like this are more interested in ratings and hype than in fact checking and counter narratives. Dozens of reporters did feature pieces on this Earhart story, mostly just repeating the PR talking-points provided to them by the History Channel. Not one of them spent even a few minutes fact-checking the key element of the story. The reporters who wrote about it did not have the knowledge-base or the desire to investigate the claims made by the filmmakers. When news organizations report on scientific and health publications, they do no better. Critical analysis is almost never a part of the coverage, and what gets covered is usually selected for it ability to attract clicks and readers; this means that reporters are happy to report on wild and outlandish health claims and studies (“low probability hypotheses”) because they fit the “man bites dog” mold, even though it’s usually the dog who bites the man.
Improbable hypotheses require incontrovertible evidence to validate them. Bayes’ theorem teaches us clearly that if you are going to accept some claim as likely true, it either needs to have a very high degree of pretest probability or very firm and sound evidence that supports it (ideally you would have both). The claim that Earhart and Noonan were in that particular photograph was a low-probability hypothesis, so the low-quality “evidence” presented in the documentary that it was them just simply wasn’t enough to matter. Most published claims in medical science are also low probability claims. Studies that report on things like the association between low levels of Vitamin D and treatment failure in Nepalese children with pneumonia (published this week in Nature) are so unlikely to be meaningfully related (that is, the claim has a low pre-study probability) that it doesn’t matter if the authors found a “statistically-significant” finding in their data or not: it’s garbage. Remember, about 80% of the medical literature published this year will eventually be disproven; you’ll have a better idea of which ones are bunk if you learn to consider pre-study probability.
Just because the data points are explained by a narrative doesn’t mean that that narrative is the only explanation for the data points. The History Channel film makers very skillfully weaved together a plot that was seemingly supported by the “evidence.” Apart from the fact that the “evidence” was false, we must also consider that many other stories and narratives contain the same data points. There is always more than one explanation (or more than one hypothesis) that explains the data. The filmmakers already had their minds made up about which story was true so they framed all the data in that context; they just as skillfully could have “proven” several others stories with the same “facts.” Narrative is everything. They made what might be called a “circumstantial case” and any good attorney could have torn it apart; the equivalent of circumstantial evidence in medical literature is the logical fallacy of assuming that correlation equals causation. Almost every piece of published scientific, medical literature is really just reporting correlation between two variables, but the authors, editors, journalists, and readers of a given article go an unwarranted step further and assume causation. One way to stop doing this is to make it a habit of always trying to think of other explanations for the findings (or other hypotheses).
Dressing things up as novel and scientific doesn’t have anything to do with whether or not they are true. The rhetorical brilliance of the History Channel documentary was how it appealed to its viewers. Every generation assumes that they are smarter than the last (they aren’t), and viewers are always gullible for some new understanding that others never had before, bolstered by new science or new techniques, without actually understanding the validity of the new science or techniques. The truth is, the hundreds of people who contemporaneously searched for Amelia Earhart and investigated her disappearance stood a far better chance of finding some actual meaningful evidence than a former Assistant Director of the FBI 80 years after the fact. But the film makers take advantage of our instinct to assume that everyone else who ever investigated the case was either dumber than us or were involved in a conspiracy to hide the truth. They claimed both of these things regarding the Earhart disappearance, and these two claims are pretty standard among conmen today. But this happens in science and medical literature all the time as well. The reader of a medical journal is much more interested in and entertained by novel claims; few people enjoy reading studies that confirm what we already know. But Bayes’ theorem tells us that what we already know is far more likely to be true than some new discovery, in a general sense. Literature that re-examines what we already know (replication studies) are almost never performed and therefore the scientific process, which requires replication, is almost never fully executed. Instead, academic careers are made the same way this History Channel documentary was made: trying to claim novelty to grab attention, and then glam the audience with pseudoscience.
People find what they want to find and then stop looking. Why was Kota Yamano able to disprove the whole show in less than 30 minutes? Speaking Japanese helps, but, more importantly, he was skeptical and didn’t believe the central premise of the show, so he looked for evidence that it was wrong, even though he was disagreeing with the “expert consensus” presented in the program. Search-satisfying is a bias employed every day in medicine: search for an article or a source that agrees with you and then stop looking. When you do that, you are likely to miss all the evidence that disagrees with you. People rarely let “the facts speak for themselves;” rather, they search for facts that agree with what they already believe (and look no more). As a rule, try to look for evidence that disagrees with what you already believe, which brings us to the last point.
Don’t seek to prove your theory, seek to disprove it by every means possible. Ultimately, this is the basis of the scientific method and the reason why so much science, including medical science, is dead wrong. This is how we avoid confirmation bias. Lazy investigators try to prove their theories; good investigators try to disprove their theories. The filmmakers didn’t once ask an expert to disprove that the photograph was of Earhart and Noonan or entertain other theories (like it was taken two years before and published in a Japanese travel book available for anyone to find on the internet). In medical literature, this sort of laziness is almost universal. You should accept something as valid only after you have doggedly attempted, in every way you can imagine, to disprove it.
Published Date : July 4, 2017
Categories : #FourTips, OB/Gyn
The Cesarean Delivery (CD) rate has dropped for a couple of years in a row now after increasing every year since about 1996. Cesarean delivery is associated with an increased risk of maternal death. Maternal death in the United States has been increasing since 1987, in tandem with the CD rate. Unnecessary Cesareans are now an epidemic, and, unfortunately, young obstetricians have grown up in a culture where almost anything is a reason to do a Cesarean. This cultural change is difficult to fight against. The medicolegal environment has created an environment where CD feels like the safe way out of most situations where the physician is even slightly uncomfortable. Axioms like, “Let’s cut our way out of this mess,” “You never get sued for a Cesarean,” or “Don’t back yourself into either a difficult vaginal or a difficult cesarean delivery” encourage a cut-everyone atmosphere. The phrase “Healthy mother, healthy baby” has been perverted to imply that a Cesarean is the means by which both are supplied, even though maternal and fetal outcomes are both consistently worse with Cesarean compared to vaginal delivery.
Fortunately, most of us recognize that the rate of CD must decline in order to combat the increasing rate of maternal mortality in the United States and improve perinatal outcomes. Here are four tips to lower your Cesarean delivery rate.
1. Use modern labor guidelines.
A great deal of progress has been made in recent years that has transformed traditional guidelines for labor management to reflect current scientific evidence. This requires Obstetricians to fundamentally change their practice patterns. The first Obstetric Care Consensus document, “Safe Prevention of the Primary Cesarean Delivery,” published in March 2014, outlines many of these needed changes, though Obstetricians as a whole have not embraced the new guidelines (as an aside, I have, and my primary CD rate in the last 12 months was 6.2% among all patients). Among the most important and transformative changes:
These changes were implemented among 200 nulliparous women with singleton, term, pregnancies who were induced or augmented and compared to a group of matched women before the new guidelines. The authors reduced their primary cesarean delivery rate among these women from 26.9% to 18.8%, with a reduction in composite morbidity by 34%. The diagnosis of “arrest of dilation” occurring before 6 cm went from 7.1% to 1.1%. This was among only nulliparous women who received augmentation or induction, meaning that if you deliver about 100 babies per year, you should expect to do a Cesarean for arrest of dilation before 6 cm in a nulliparous woman only about once every four years.
2. Don’t induce women with unfavorable cervices unless they really need it.
Labor arrest is the reason for about 1/3 of primary CDs. Most of those can be avoided with Tip #1. But induction of labor among women with unfavorable cervices, particularly nulliparous women, still roughly doubles the risk of Cesarean (in studies conducted with CD rates under 30%). So don’t induce women with unfavorable cervices, particularly nulliparous women, unless you have a medical indication or unless they have reached 41 weeks. When you do induce them, use modern labor guidelines and best practices for induction (like cervical ripening with a balloon plus misoprostol or a balloon plus oxytocin) and be patient: if you are going to induce someone with an unfavorable cervix, count on it taking at least 24 hours. The Guideline also states:
3. Stop over-treating Category 2 fetal heart tracings.
Rapid delivery is indicated for non-resolving Category 3 fetal heart tracings (absent variability plus recurrent late or variable decelerations, bradycardia, or a sinusoidal pattern); this means operative vaginal delivery if she is a candidate or Cesarean delivery if she is not. Category 3 fetal tracings are rare; in fact they occur in less than 1 in 1000 patients. Yet about 23% of primary Cesareans are done for “non-reassuring fetal heart tracings.” This means they are being done almost exclusively for Category 2 tracings. Use of amnioinfusion for recurrent variable decelerations may reduce the risk of CD, as well as use of scalp stimulation to gain reassurance when decreased fetal heart rate variability is present. Using a standardized approach to treatment of Category 2 tracings can significantly reduce this number. One such approach was suggested by Clark et al. in 2013 and is shown below:
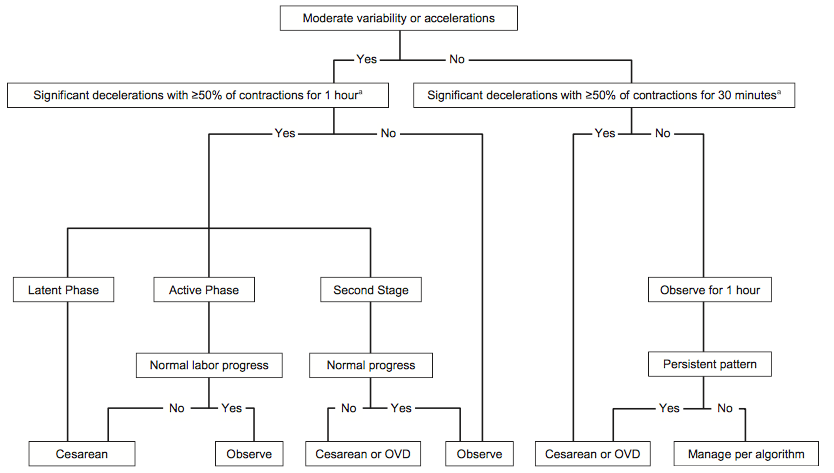
This type of approach to fetal heart tracings should mean that if you deliver 100 babies per year, you would perform one or two Cesareans each year for an abnormal or indeterminate fetal tracing.
4. Support a Trial of Labor After Cesarean (TOLAC).
Almost 1/3 of all Cesareans done are repeat Cesareans. The truly catastrophic outcomes seen with Cesarean delivery tend to occur not with the first Cesarean, but with subsequent Cesareans or trials of labor. If there are fewer primary Cesareans done, then in time there will be fewer repeat Cesareans done and this can have a large impact on outcomes like maternal mortality. At the same time, supporting a woman’s choice to attempt a TOLAC is an important element of reducing the total Cesarean rate and the risk of maternal mortality. Women are 3.5x as likely to die with an elective repeat CD than with a vaginal birth after Cesarean (VBAC). VBAC success rates also increase substantially by using modern labor guidelines, making even more women good candidates for a TOLAC, based on their probability of success.
What else?
Don’t perform a Cesarean on women just because they have twins. Twins pregnancies delivered vaginally have consistently better outcomes than those born by Cesarean.
Screen for malpresentation at 36 weeks and offer all women external cephalic version (ECV) by 37 weeks. There is no excuse to not know the presenting part in term pregnancies and most women are excellent candidates for external cephalic version.
Don’t recommend Cesarean to women for babies weighing less than 5,000 grams (11 lbs) or 4,500 grams (9 lbs, 14 ounces) in diabetic mothers. Studies have failed to show benefit in weights smaller than this for reducing the risk of permanent injury to newborns related to birth trauma.
Give women time to push! Give multiparous women at least two hours and nulliparous women at least three hours to push, with more time if they have a dense epidural.
Change the culture. All of these changes require significant culture changes and teamwork among the physicians, staff, and nurses. Many hospitals have a culture that doesn’t tolerate vaginal delivery: too many inductions, too little patience, no TOLACs, no ECVs, no one allowed to push for more than about an hour, everyone is always in crisis mode, etc. Too many people describe an 8-pound baby as “big” and too many residents today have never seen a woman push for three hours or more. Every hospital should review every primary Cesarean in a formal manner and do a root cause analysis to see how it might have been avoided. Every physician should know her primary Cesarean rate and should stop making excuses for it; we all treat high risk patients, obese patients, diabetic, patients, etc. Cesarean delivery rates vary from about 7% to about 70% from hospital to hospital and this variation is unnecessary and harmful. Let’s change it!
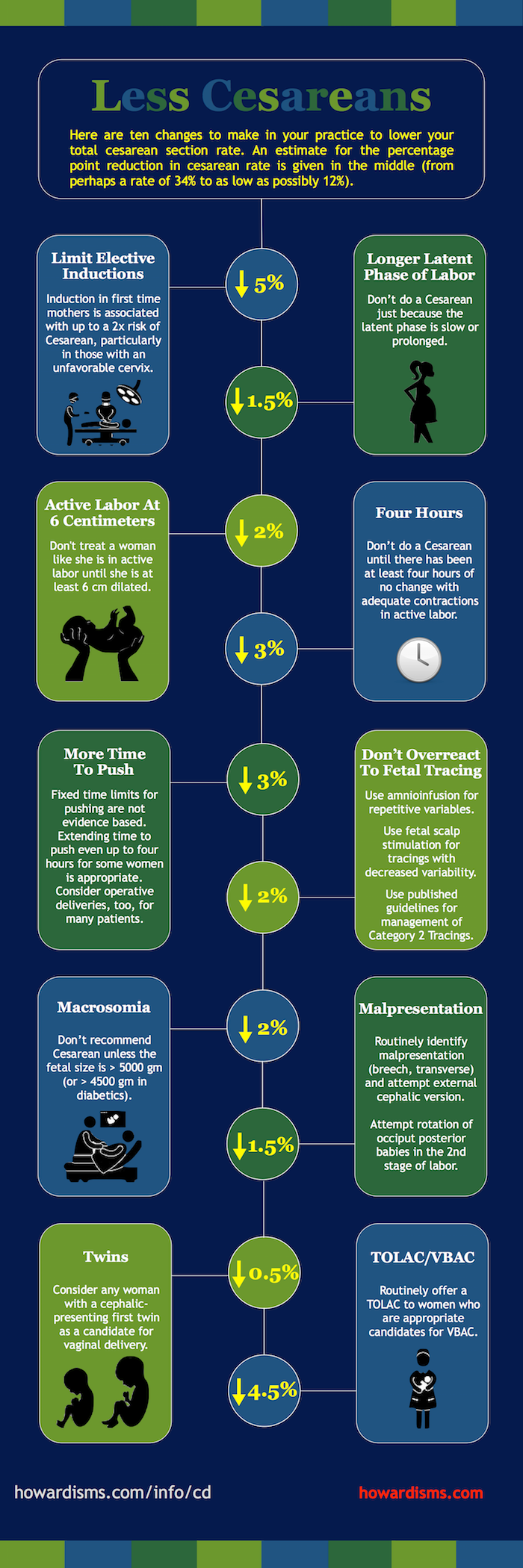
Published Date : June 28, 2017
Categories : #FourTips, OB/Gyn
Complaints of vaginal irritation and/or vaginal discharge are very common in ambulatory settings, particularly in gynecology offices. Bacterial vaginosis, candidiasis, and trichomoniasis account for about 70% of these complaints. Patients who present with these symptoms are frequently over-treated and misdiagnosed. Those with recurrent symptoms are especially challenging. Here are four tips for correctly diagnosing women with symptoms of vaginitis.

1. Check the pH.
Testing the vaginal pH is often under-utilized in clinical practice. Many providers either rely almost exclusively upon history for the diagnosis of vaginitis or other ancillary tests that are non-specific. The differential diagnosis for symptoms of vaginal irritation and discharge is long and includes physiologic discharge, herpes, atrophic vaginitis, gonorrhea, chlamydia, desquamative inflammatory vaginitis, vulvodynia, vulvar dystrophy, vulvar dermatitis, retained foreign bodies, non-Candida albicans yeast infections, in addition to the big three: vulvovaginal candidiasis, bacterial vaginosis, and trichomoniasis.
Determining the vaginal pH is a valuable first step in narrowing down the differential diagnosis. A normal vaginal pH is < 4.7; anything ≥ 4.7 is considered abnormal. Women with vulvovaginal candidiasis, genital herpes, vulvodynia, vulvar dermatitis, and a physiologic discharge will have a normal vaginal pH. Women with bacterial vaginosis, atrophic vaginitis, desquamative inflammatory vaginitis, cervicitis, and other conditions, will have an elevated pH. The presence of blood, semen, cervical mucus, and amniotic fluid will also result in an elevated vaginal pH. For women with trichomoniasis, the vaginal pH may be normal or abnormal.
In addition to helping narrow down the differential, knowing the vaginal pH is also essential to diagnosing bacterial vaginosis (see Tip #2).
2. Don’t rely on a test to diagnose BV.
BV is a clinical diagnosis; it should not be diagnosed based upon a test result. This occurs sometimes with Pap smear results that show a shift in flora consistent with BV and it also occurs frequently today with PCR based tests for Gardnerella vaginalis. But the clinical diagnosis of BV should be based on Amsel’s criteria, which requires that the patient have a three of four findings:
The presence of Gardnerella vaginalis detected by culture or PCR does not indicate that the patient has BV; similarly, the absence of Gardnerella vaginalis does not mean the the patient doesn’t have BV. Women with a clinical diagnosis of BV may have infection with any of a number of bacterial species, including Atopobium vaginae, Prevotella, Bacteroides, Peptostreptococcus, and several others. Reliance upon the presence of Gardnerella vaginalis for diagnosis may lead to under-diagnosis of BV due to the condition being caused by other bacteria. Unfortunately, as these tests have become commercially available they’ve been introduced into practice without scientific evidence. Providers increasingly forego valuable clinical testing, skipping not only the vaginal pH but also the whiff test. The whiff test will usually be positive only with bacterial vaginosis and, in some cases, trichomoniasis.
3. Don’t treat normal discharge.
For many providers, any complaint of a white and bothersome discharge is treated as yeast. If the symptoms don’t improve, then recurrent or resistant disease is suspected and treated. But in many cases the discharge that’s noticed is normal and physiologic. Physiological discharge ranges from a clear mucus in the mid cycle to a thick white discharge at other times that is frequently mistaken for candidiasis. During menses, the discharge may even look purulent and be mistaken for cervicitis. Physiologic discharge is a diagnosis of exclusion. The patient should have a normal vaginal pH, a negative whiff test, and Lactobacillus present on saline microscopy. The amount of discharge and consistency will vary with different methods of hormonal birth control. Many patients will need to see evidence of a negative culture to be convinced that their discharge is normal. About 10% of women with chronic or recurrent vaginal complaints simply have physiologic discharge.
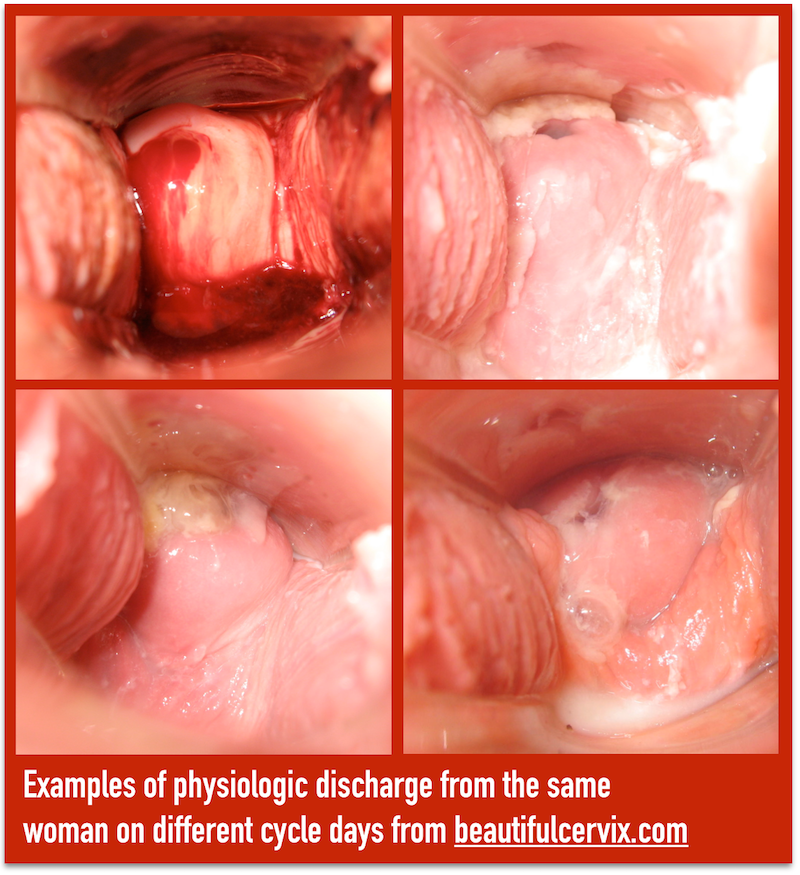
Since physiologic discharge is a diagnosis of exclusion, don’t forget to exclude chlamydia, gonorrhea, trichomoniasis, and at least consider rare causes of chronic discharge like vesicovaginal fistula or fallopian tube cancers. Don’t get in the mindset that everything that is white is yeast, everything yellow-gray is BV, and everything green is trichomoniasis, or in the mindset that everything that itches is yeast or everything that smells like fish is BV. These clues help aid in diagnosis, but basing treatment primarily on these clinical symptoms often leads to the wrong diagnosis. In some cases, this means that patients are convinced that their normal cervical discharge is a yeast infection requiring treatment; in other cases, it means that patients believe that their atrophic vaginitis or lichen sclerosis is simply a yeast infection. Patient are harmed in both cases.
4. Think outside the box.
Most misdiagnosis happens because of a limited differential diagnosis followed by premature closure or confirmation bias. For example, a patient presents with itching and the physician thinks yeast. She then sees thick white discharge on exam and treats the patient for yeast, ignoring the fact that there are no yeast present on wet mount. The treatment may be appropriate: it is possible that there are no yeast on the wet mount due to a false negative test. But it is also possible that the thick white discharge is a physiologic discharge and that there is another, undiagnosed reason for the itching. More than 1/3 of women who present with symptoms of vaginitis don’t have one of the big three (trich, BV, yeast). This means that if you always seem to be diagnosing one of those three, you are very often wrong. So, consider the possibilities:
What else?
Published Date : June 5, 2017
Categories : #FourTips, OB/Gyn
The initial trocar placement at the time of laparoscopic surgery is the most important step: 50% of complications that occur during laparoscopic surgery occur with the initial laparoscopic puncture. Here are four tips to reduce the risk of injury when making the initial entry.
1. Use a direct entry optical trocar, preferably one that insufflates upon immediate perforation of the peritoneum.
For most surgeons who want to improve safety at the time of initial laparoscopic entry, the focus is on the method of entry. The most common choices are the open or cut-down method (Hasson method), pre-insufflation with a Veress needle followed by trocar placement, or direct entry with or without an optical trocar.
The debate over which technique is best centers around two main types of injury: major vascular injury and bowel injury. Both types of injury are rare but dozens of studies, both prospective and retrospective, have been done to give us some numbers regarding the injury rate.
Molloy et al. performed a meta-analysis of 51 studies performed before the year 2000. They found the following rates of injury per 1000 cases:
| Veress | Open | Direct | |
| Bowel injury | 0.4 | 1.1 | 0.5 |
| Vascular injury | 0.4 | 0 | 0 |
| Combined injury | 0.8 | 1.1 | 0.5 |
These rates of injury are basically the same in the prospective studies as well. When patients were randomized prospectively to open vs the direct entry techniques (eliminating the selection bias for patients at high risk for bowel injury), the following rates were found per 1000 patients:
| Open | Direct | |
| Bowel injury | 0.82 | 0.31 |
| Vascular injury | 0 | 0 |
| Combined injury | 0.82 | 0.31 |
So, the direct entry is superior even in randomized trials.
Interestingly, virtually every vascular injury in the dozens of studies available occurred with Veress needle entry. Both open and direct entry techniques virtually eliminate the risk of major vascular injury. But the open technique, first described by Hasson in 1971, poses a relative risk of 2.6-fold for bowel injury as compared to the direct entry technique. The open technique was created to combat vascular injuries that were occurring at the time of Veress needle placement, not to reduce the risk of bowel injury. Today, unfortunately, many surgeons assume that it has the benefit of reducing bowel injuries, but this is not supported by evidence.
Modern direct entry trocars are optical trocars, which allow the surgeon to survey the layers of tissue during the entry. This should lead to a further reduction in injuries as well, particularly with trocars that insufflate as soon as the peritoneum is punctured. Direct entry also carries a lower risk of failed laparoscopy compared to use of the Veress needle, and failed entry dramatically increases the risk of visceral and vascular injuries, usually because the surgeon becomes more aggressive with the angle of insertion and depth while entry becomes more difficult due to preperitoneal insufflation. When three attempts or more are needed, half of cases suffer a complication ranging from extraperitoneal insufflation to omental, bowel, or vascular injuries.
There are some other advantages of direct entry:
The clear winner seems to be direct entry laparoscopy with an optical trocar. This contradicts years of traditional teaching and what purports to be common sense regarding avoidance of major injuries at the time of initial port placement. Unfortunately, what the evidence holds out as the safest option is also the least used, with only about 10% of surgeons/gynecologists routinely using this technique.
2. Place your incision deep in the umbilicus.
The base of the umbilicus is the thinnest entry point into the peritoneal cavity. Traditionally, laparoscopic incisions have been placed infra-umbilically for ease of closure and ease of dissection. But one advantage of using direct optical entry is that dissection and closure with suture are unnecessary. This allows placement of the initial incision in the ideal place, which is at the base of the umbilicus. The abdominal wall is thinnest at this point and creates the ideal geometry for successful placement.
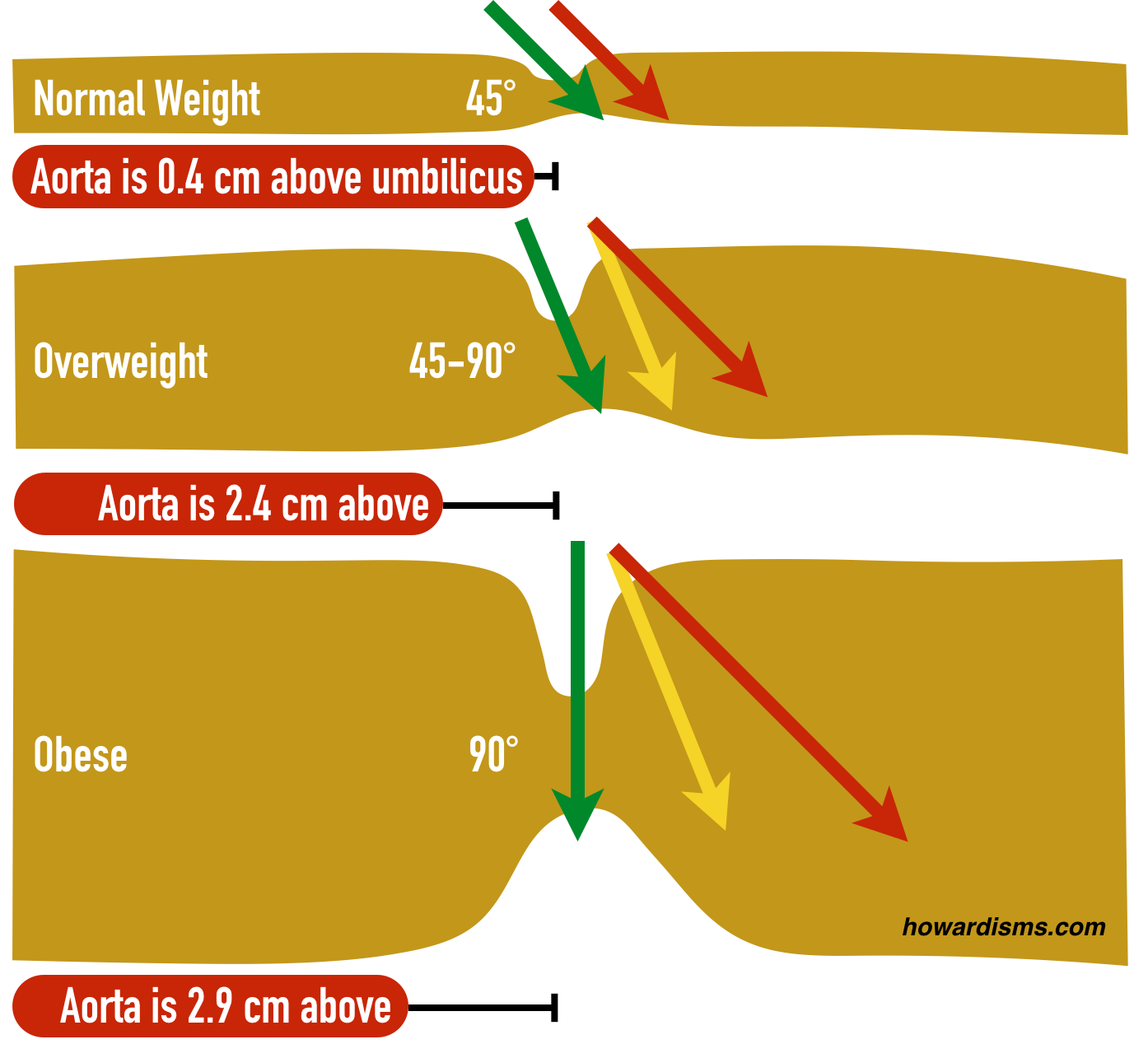
In the picture above, the green arrow represents the ideal trocar placement location and angle for each body type. A normal length trocar works usually even for very obese patients as long as the correct location is being used. When the trocar is placed below the umbilicus or at the wrong angle (yellow and red arrows), then the distance to be traversed increases dramatically and the so does the risk of failed laparoscopy.
3. Know where the bifurcation of the aorta is in relationship to the umbilicus and use the correct entry angle for the patient’s size.
Also illustrated in the diagram above is the location of the aorta. The bifurcation of the aorta is 0.4 cm cephalad to the base of the umbilicus in a normal weight woman. Practice locating the bifurcation by placing your finger in the umbilicus and feeling for the pulsation the aorta. In thin women, the proximity of the aorta demands angling the trocar away from it to avoid injury, usually at about 45°. As the woman’s weight increases, the umbilicus is pulled downward in relation to the bifurcation; at the same time, the thickness of the tissue increases so that the angle must become closer to 90°. For obese women, the bifurcation is an average of 2.9 cm cephalad to the base of the umbilicus so the trocar can go straight in, at a 90° angle. Overweight women are in between these two extremes, and so too the angle of the trocar is usually in between.
Also, make sure that the angle of insertion is parallel to the long axis of the body; even slight lateral angulation can lead to the trocar damaging the common iliac or internal iliac vessels (green is good, yellow is bad).
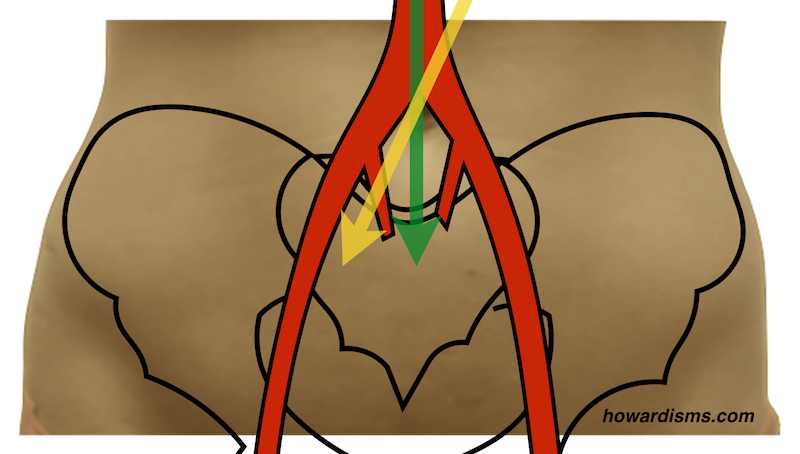
4. Use Palmer’s point if her risk of umbilical adhesions is high.
Most bowel injuries happen because of adhesions to the abdominal wall near the base of the umbilicus. In fact, more than half of bowel injuries with direct entry occur in patients with previous vertical abdominal laparotomy incisions or multiple previous infra- or intra-umbilical incisions. Use of an alternative site, such as Palmer’s point, 3 cm below the costal margin on the left side at the midclavicular line, would theoretically reduce the rate of bowel injury with the direct entry method by half. Consider this location for patients with risk factors for umbilical adhesions, chiefly a prior vertical incision or 3 or more prior umbilical punctures. But remember, don’t use Palmer’s point if the patient has had prior gastric surgery. Always decompress the stomach first and palpate for splenomegaly.
What else?
Make sure your skin incision is big enough; you don’t need to fight skin friction on the way in. Use a back-and-forth twisting motion with the trocar to break the skin friction. Elevate the abdominal wall below the umbilicus with your hand or use towel clamps at the umbilicus if necessary. Don’t place the patient in Trendelenberg’s position while making your initial puncture; this will shift the geometry of the umbilicus-to-aortic bifurcation in an unfavorable way and make your needed angle of entry much more acute.
Published Date : May 26, 2017
Categories : #FourTips, OB/Gyn
Postpartum sterilization is a relatively low-cost and convenient option for many women, but it is too often under-utilized because many obstetricians struggle with the technique. A postpartum tubal ligation should take about ten minutes, but for many surgeons it turns into an unnecessarily longer procedure as they struggle to locate the fallopian tubes. Here are four tips (and a video) to make it easier.
1. Do the tubal as soon as possible after delivery.
In many hospitals, it’s customary to do a postpartum tubal the day after delivery or even two days after delivery. The longer it’s been since the time of delivery, the smaller the uterus. The smaller the uterus, the further it is from the umbilicus. There’s no good reason not to do a postpartum tubal ligation immediately after the delivery. This usually means waiting about an hour after delivery to make sure that the mother is stable, but waiting further only makes the case harder. Any opportunity to do the tubal ligation the day of delivery should be taken. Not only will the case be easier, but there is a greater chance that she will be able to use her epidural for anesthesia and that it will provide adequate pain relief for the surgery. This also means that the epidural can be removed that same day, rather than indwelling overnight. Obviously, there are circumstances where, for logistical reasons, the tubal ligation can’t be done immediately; either the surgeon or an operating room may not be available. In any event, every effort should be made to do it as soon as possible, even if it’s first thing the next morning. Waiting at least an hour provides the mother with an opportunity to bond with the baby during the Golden Hour. When she comes back, the baby will have had its newborn assessment and other care completed ready to greet mom. Plus, the mother will be awake without prolonged recovery associated with general anesthesia and ready to go. Waiting until the next day usually means several hours apart and recovery from general anesthetic.
2. Make a smaller incision.
When surgeons struggle doing a postpartum tubal ligation, they quickly start making bigger and bigger incisions. I’ve seen incisions under the unbilicus that are 3 or even 4 cm long in an attempt to make the case easier. If you’re using good technique, there’s no need to make a bigger incision. In fact, you’ll have a happier patient if you can contain the incision completely within the umbilicus or in the natural folds of the umbilicus. Usually an incision that’s less than 15 mm to 18 mm is able to be contained within the umbilical folds. As a rule, if you can stick one finger in the incision, even your pinky finger, then you can do a postpartum tubal through the incision. The key to making the case easier isn’t making a bigger incision; the key is to use better technique. Not only will your patient be happier with the cosmetic result, but you will save time. This type of incision can be closed with a simple figure-of-eight suture in the fascia and glue on the skin, much like a large, laparoscopic trocar incision. A curvilinear incision along the lower rim of the umbilicus is usually adequate. If you find that this is too small, the incision can be made slightly larger by extending the edges cephalad to create a U shaped incision.

3. Use a sucker tip to elevate the tube.
If you’re making a smaller incision, then you need a way of elevating the tube to the incision that doesn’t require extensive retraction or instrumentation in the peritoneal cavity. This is where the sucker tip comes into play. Make sure the tip is not hooked up to actual suction; then you use the tip to elevate the tube to the incision where it can be grasped with a Babcock clamp. Place the tip in the incision on top of the uterus, then slide it over the fundus with a fair amount of pressure until it slides up behind the uterus. This will usually push any bowel or omentum out of the way. Once the tip is placed firmly behind the uterus, draw the tip laterally with moderate constant pressure while removing the suction tip up and out of the umbilicus so that eventually whatever is sitting on top of the tip is brought up to the incision. You won’t see the tube until you get to the incision, and that’s okay: this is all done by feel. If you’ve done this well, then by the time the tip makes it to the incision the fallopian tube will be sitting immediately on top of it. You can then grasp the fallopian tube with a Babcock clamp and the rest is easy. If you don’t have the tube on the tip, then you might have the round ligament instead. This is still useful. Grasping the round ligament may allow you to use Babcock clamps to walk towards the fallopian tube. Oftentimes, what comes up on the tip is omentum. It’s the omentum that frustrates surgeons as they try to elevate the tube to the incision. The fourth tip is the best way to get the omentum out-of-the-way.

The sucker tip has hooked the tube and pulled it up to the incision in the picture above.
4. Use the table to your advantage.
Don’t be afraid to put the patient into Trendelenburg position, even steep Trendelenburg position, to get the omentum and bowel out of the way. This is by far the best way to deal with pesky omentum that keeps making the case more difficult. You can also airplane the patient to the left or right side. If you’re working on the right tube, you might airplane the patient to the left side, for example. With appropriate bed positioning, the case is usually made dramatically easier.
What else?
If you’re right-handed, stand on the patient’s left side for this procedure. This will allow you to use your right hand for the most crucial part of the case, which is the manipulation of the suction tip. If you’re left-handed, then stand on the patient’s right side.
Use a suture on a UR-6 needle to close the fascia; the acute angle of the needle will make it easier to take the sharp turn you need without putting the bowel at risk of injury.
Always make sure you identify the fallopian tube with certainty by walking down to the fimbriated portion of the tube. Then come back to about 3 cm from the cornua to perform the partial salpingectomy.
When you excise a portion of the tube, look for the “hotdog sign.” By looking at the cut portion on end, you should be able to see the inner tube (the wiener) sticking out of the surrounding tissue (the bun). This will decrease the chance that you ever accidentally resect a piece of round ligament or other connective tissue by accident.
Check out the video to see these tips in action.