
There are no free lunches in life; sorry. Everything has its pluses and minuses. There are no medicines that are completely safe, and there is no life without medicines that is completely safe. All of us weigh risks and benefits every time we make a decision: what to eat for lunch, what car to drive, whether to ensure our farm equipment, etc. That’s life.
Every single decision in medicine involves such risk vs. benefit calculations. Most doctors (and patients) are bad at this. We exaggerate the benefits and we minimize the risks if we are considering something we are already inclined to do, and we do the opposite if it’s something that we don’t want to do.
I spend a lot of my time trying to reframe risks and benefits in a way that my patients can understand so that they can make better decisions. When it comes to birth control, many patients present with a ton of preconceptions (most of which are wrong). They inherit these misconceptions from their moms, girlfriends, doctors, Facebook, Twitter, advertising agencies, mischevious lawyers, etc.
When it comes to birth control, I naturally want my patients to use something that is highly effective, safe, convenient, and cost-effective (but my patients often, unintentionally, want the opposite). In real terms, I want my patients to use a LARC or long-acting, reversible contraception (like the Mirena IUD) but often they just want The Pill. Society has programmed women to believe that The Pill = birth control and that IUDs are barbaric contraptions that sterilize women.
Almost daily, I am told that IUDs cause a litany of horrific problems: infertility, pelvic infections, unnecessary hysterectomies, pain, baldness, ovarian cysts, ectopic pregnancies, miscarriages, etc. Faced with such daunting and dire potential risks, the patient will instead be happy with The Pill, as if The Pill is the safest thing ever made by man.
A good trick is to reframe risks and benefits in terms of absolute risks, not relative risks. Patients (and doctors) can understand real percentages better than relative risks or odds ratios. I also need to tell my patients about outcomes that they might not have considered but which are, nevertheless, very important.
The chart below demonstrates how I do this when comparing The Pill to medicated IUDs. I tell the patient to imagine that I prescribe The Pill to 1000 women today and I put a medicated IUD in another 1000 women. What will happen over 5 years? (yes, I tell them all of this information)
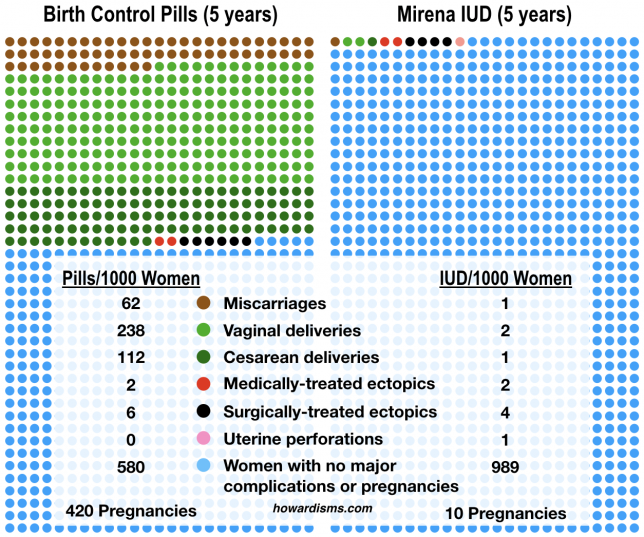
These numbers are accurate, based upon our best available data. The IUD is associated with the fewest miscarriages, the fewest vaginal and cesarean deliveries of normal pregnancies, the fewest ectopic pregnancies, and the fewest surgeries performed for ectopic pregnancies. But, alas, there is that 1 per 1000 risk of uterine perforation (which can sometimes result in a surgery to remove the device, though that surgery isn’t medically necessary for any IUD except the ParaGard and the surgery doesn’t result in permanent damage).
Put another way, the women who choose the IUD deliver 3 children over 5 years while the women who choose The Pill have 350 children. For the IUD users, 7 women will have surgeries (1 for the perforation, 1 Cesarean, and 4 for treatment of ectopics) while over 140 women who take The Pill will have surgeries (112 Cesareans, 6 for treatment of ectopics, and the rest for treatment of incomplete abortions).
Bottom line: with the IUD I make 98.9% of women happy but with The Pill only 58%.
Of course, the data in the chart doesn’t tell the whole story, but, when presented correctly, can be very compelling. It’s all about redirecting false narratives. The false narrative is that IUDs are risky and dangerous, but the truth is that this narrative should be ascribed to The Pill.
Additional details to emphasize:
- Women who use The Pill are 20 times as likely to die as IUD users (mainly from thromboembolism).
- The IUD is convenient and worry-free.
- The IUD has almost no contraindications or drug-to-drug interactions.
- The medicated IUDs have a greater chance of eumenorrhea (periods she’ll be happy with) than The Pill.
- IUDs don’t cause acne or ovarian cysts or pelvic pain, but not taking The Pill can cause those things; many women blame the IUD for problems they have that were once surreptitiously being treated by The Pill. If this happens, just give them The Pill back (and leave the IUD in place).
- IUDs have no effect on mood, weight gain, or breastfeeding.
Sometimes, the complete counseling conversation takes well over 30 minutes, but it’s important. The quality of my counseling may be the difference in a young woman graduating high school or college or living in poverty or on government assistance for the rest of her life. Effective birth control is tremendously important as a social determinant.
What’s your LARC utilization rate? If it’s less than 50%, you’re not trying…